

Treatment With 25-Hydroxyvitamin D3 (Calcifediol) Is Associated With a Reduction in the Blood Neutrophil-to-Lymphocyte Ratio Marker of Disease Severity in Hospitalized Patients With COVID-19: A Pilot Multicenter, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial
- PMID: 34653608
- PMCID: PMC8511889
- DOI: 10.1016/j.eprac.2021.09.016
Treatment With 25-Hydroxyvitamin D3 (Calcifediol) Is Associated With a Reduction in the Blood Neutrophil-to-Lymphocyte Ratio Marker of Disease Severity in Hospitalized Patients With COVID-19: A Pilot Multicenter, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial
Abstract
Objective: The goal of this randomized, double-blinded, placebo-controlled clinical trial was to investigate the therapeutic efficacy of oral 25-hydroxyvitamin D3 (25(OH)D3) in improving vitamin D status in vitamin D-deficient/vitamin D-insufficient patients infected with the SARS-CoV-2 (COVID-19) virus.
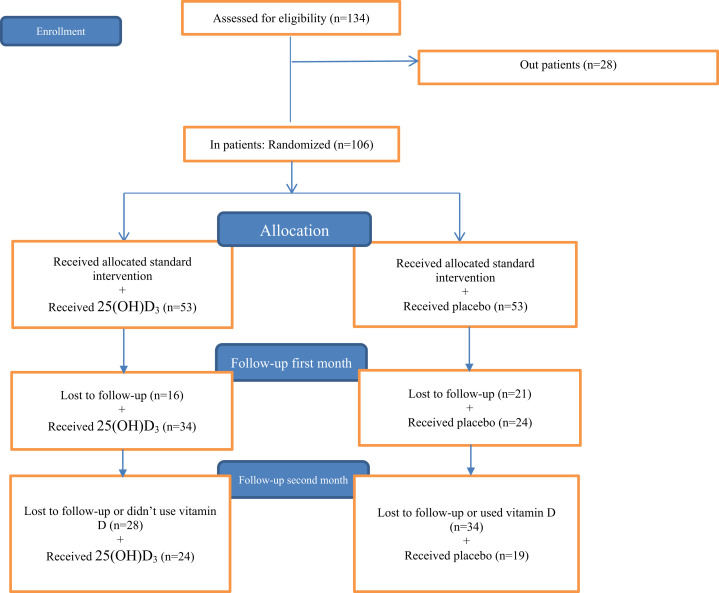
Methods: This is a multicenter, randomized, double-blinded, placebo-controlled clinical trial. Participants were recruited from 3 hospitals that are affiliated to [Institution Blinded for Review] and [Institution Blinded for Review].
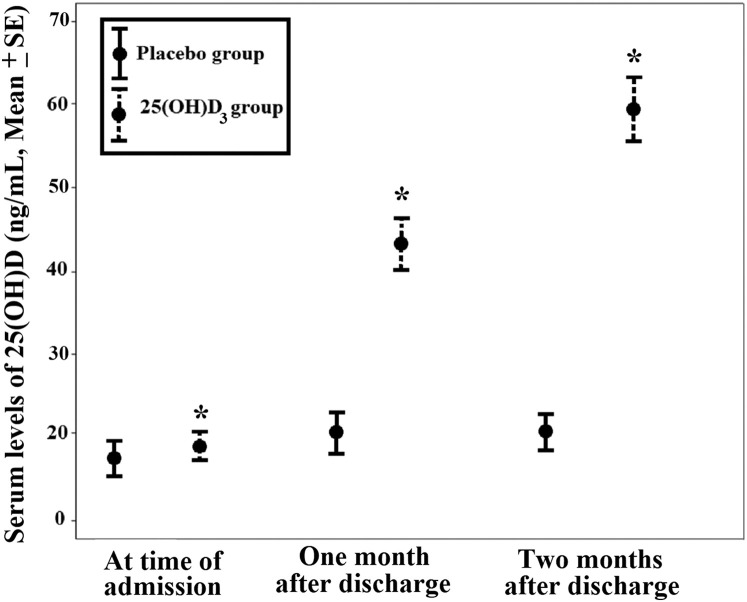
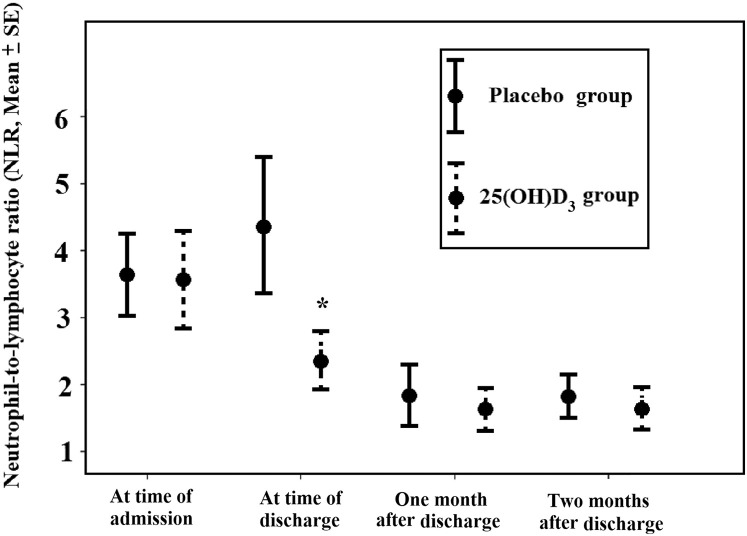
Results: A total 106 hospitalized patients who had a circulating 25(OH)D3 concentration of <30 ng/mL were enrolled in this study. Within 30 and 60 days, 76.4% (26 of 34) and 100% (24 of 24) of the patients who received 25(OH)D3 had a sufficient circulating 25(OH)D3 concentration, whereas ≤12.5% of the patients in the placebo group had a sufficient circulating 25(OH)D3 concentration during the 2-month follow-up. We observed an overall lower trend for hospitalization, intensive care unit duration, need for ventilator assistance, and mortality in the 25(OH)D3 group compared with that in the placebo group, but differences were not statistically significant. Treatment with oral 25(OH)D3 was associated with a significant increase in the lymphocyte percentage and decrease in the neutrophil-to-lymphocyte ratio in the patients. The lower neutrophil-to-lymphocyte ratio was significantly associated with reduced intensive care unit admission days and mortality.
Conclusion: Our analysis indicated that oral 25(OH)D3 was able to correct vitamin D deficiency/insufficiency in patients with COVID-19 that resulted in improved immune function by increasing blood lymphocyte percentage. Randomized controlled trials with a larger sample size and higher dose of 25(OH)D3 may be needed to confirm the potential effect of 25(OH)D3 on reducing clinical outcomes in patients with COVID-19.
Keywords: 25-hydroxyvitamin D(3); COVID-19; lymphocyte; supplementation; viral infection; vitamin D deficiency.
Copyright © 2021 AACE. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- COVID 19 information. Accessed Month DD, YYYY. https://covid19.continualflight.com/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
