

Exploring antibiotic prescribing in public and private primary care settings in Singapore: a qualitative analysis informing theory and evidence-based planning for value-driven intervention design
- PMID: 34654368
- PMCID: PMC8519324
- DOI: 10.1186/s12875-021-01556-z
Exploring antibiotic prescribing in public and private primary care settings in Singapore: a qualitative analysis informing theory and evidence-based planning for value-driven intervention design
Abstract
Background: Singapore's healthcare system presents an ideal context to learn from diverse public and private operational models and funding systems.
Aim: To explore processes underpinning decision-making for antibiotic prescribing, by considering doctors' experiences in different primary care settings.
Methods: Thirty semi-structured interviews were conducted with 17 doctors working in publicly funded primary care clinics (polyclinics) and 13 general practitioners (GP) working in private practices (solo, small and large). Data were analysed using applied thematic analysis following realist principles, synthesised into a theoretical model, informing solutions to appropriate antibiotic prescribing.
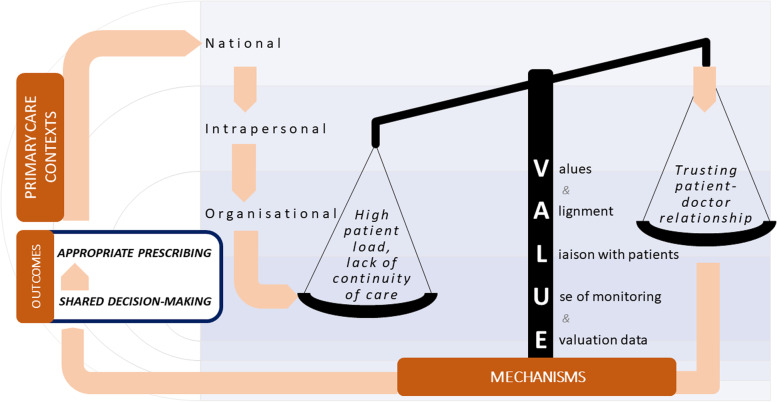
Results: Given Singapore's lack of national guidelines for antibiotic prescribing in primary care, practices are currently non-standardised. Themes contributing to optimal prescribing related first and foremost to personal valuing of reduction in antimicrobial resistance (AMR) which was enabled further by organisational culture creating and sustaining such values, and if patients were convinced of these too. Building trusting patient-doctor relationships, supported by reasonable patient loads among other factors were consistently observed to allow shared decision-making enabling optimal prescribing. Transparency and applying data to inform practice was a minority theme, nevertheless underpinning all levels of optimal care delivery. These themes are synthesised into the VALUE model proposed for guiding interventions to improve antibiotic prescribing practices. These should aim to reinforce intrapersonal Values consistent with prioritising AMR reduction, and Aligning organisational culture to these by leveraging standardised guidelines and interpersonal intervention tools. Such interventions should account for the wider systemic constraints experienced in publicly funded high patient turnover institutions, or private clinics with transactional models of care. Thus, ultimately a focus on Liaison between patient and doctor is crucial. For instance, building in adequate consultation time and props as discussion aids, or quick turnover communication tools in time-constrained settings. Message consistency will ultimately improve trust, helping to enable shared decision-making. Lastly, Use of monitoring data to track and Evaluate antibiotic prescribing using meaningful indicators, that account for the role of shared decision-making can also be leveraged for change.
Conclusions: These VALUE dimensions are recommended as potentially transferable to diverse contexts, and the model as implementation tool to be tested empirically and updated accordingly.
Keywords: Antibiotic prescribing; Antimicrobial stewardship; Primary health care doctors; Qualitative research; VALUE model for appropriate antibiotic prescribing in primary care.
© 2021. The Author(s).
Conflict of interest statement
All the authors declare no competing interests.
Figures
Similar articles
-
General practitioners' accounts of negotiating antibiotic prescribing decisions with patients: a qualitative study on what influences antibiotic prescribing in low, medium and high prescribing practices.BMC Fam Pract. 2019 Dec 10;20(1):172. doi: 10.1186/s12875-019-1065-x. BMC Fam Pract. 2019. PMID: 31823739 Free PMC article.
-
"Antibiotics are for everyone, our past and our future generations, right? If antibiotics are dead, we will be in big trouble": Building on community values for public engagement on appropriate use of antibiotics in Singapore.Front Public Health. 2022 Sep 30;10:1001282. doi: 10.3389/fpubh.2022.1001282. eCollection 2022. Front Public Health. 2022. PMID: 36249259 Free PMC article.
-
Hospitalised patients as stewards of their own antibiotic therapy: a qualitative analysis informing the strategic design of interventions to encourage shared decision-making in tertiary hospital settings in Singapore.Front Public Health. 2024 Jul 31;12:1347764. doi: 10.3389/fpubh.2024.1347764. eCollection 2024. Front Public Health. 2024. PMID: 39145162 Free PMC article.
-
A qualitative literature review exploring the drivers influencing antibiotic over-prescribing by GPs in primary care and recommendations to reduce unnecessary prescribing.Perspect Public Health. 2021 Jan;141(1):19-27. doi: 10.1177/1757913919879183. Epub 2019 Oct 21. Perspect Public Health. 2021. PMID: 31633458 Review.
-
Context and general practitioner decision-making - a scoping review of contextual influence on antibiotic prescribing.BMC Fam Pract. 2021 Nov 15;22(1):225. doi: 10.1186/s12875-021-01574-x. BMC Fam Pract. 2021. PMID: 34781877 Free PMC article.
Cited by
-
Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study.Antibiotics (Basel). 2022 Jun 4;11(6):769. doi: 10.3390/antibiotics11060769. Antibiotics (Basel). 2022. PMID: 35740175 Free PMC article.
-
An exploratory mixed methods study on shared decision-making and antibiotic prescribing for pet cats and dogs in Singapore veterinary clinics.Sci Rep. 2025 Jul 2;15(1):23135. doi: 10.1038/s41598-025-04881-w. Sci Rep. 2025. PMID: 40594052 Free PMC article.
-
Factors contributing to the variation in antibiotic prescribing among primary health care physicians: a systematic review.BMC Prim Care. 2024 Jan 2;25(1):8. doi: 10.1186/s12875-023-02223-1. BMC Prim Care. 2024. PMID: 38166736 Free PMC article.
-
A One-Week Course of Levofloxacin/Dexamethasone Eye Drops: A Review on a New Approach in Managing Patients After Cataract Surgery.Ophthalmol Ther. 2022 Feb;11(1):101-111. doi: 10.1007/s40123-021-00435-1. Epub 2021 Dec 22. Ophthalmol Ther. 2022. PMID: 34936061 Free PMC article. Review.
-
Factors influencing physicians' antimicrobial prescribing decisions: A systematic review of qualitative studies.Br J Clin Pharmacol. 2025 May;91(5):1330-1351. doi: 10.1002/bcp.70011. Epub 2025 Mar 12. Br J Clin Pharmacol. 2025. PMID: 40070317 Free PMC article.
References
-
- Review on Antimicrobial Resistance . Antimicrobial resistance: tackling a crisis for the health and wealth of nations. 2014.
-
- World Health Organization . Global action plan on antimicrobial resistance. 2015. - PubMed
-
- Dellit TH, Owens RC, McGowan JE, Gerding DN, Weinstein RA, Burke JP, Huskins WC, Paterson DL, Fishman NO, Carpenter CF, Brennan PJ, Billeter M, Hooton TM. Infectious Diseases Society of America and the Society of Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159–177. doi: 10.1086/510393. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
