

Influence of bone anatomical morphology of mandibular molars on dental implant based on CBCT
- PMID: 34654414
- PMCID: PMC8518329
- DOI: 10.1186/s12903-021-01888-3
Influence of bone anatomical morphology of mandibular molars on dental implant based on CBCT
Abstract
Background: To apply CBCT to investigate the anatomical relationship between the mandibular molar and alveolar bone, aimed to provide clinical guidelines for the design of implant restoration.
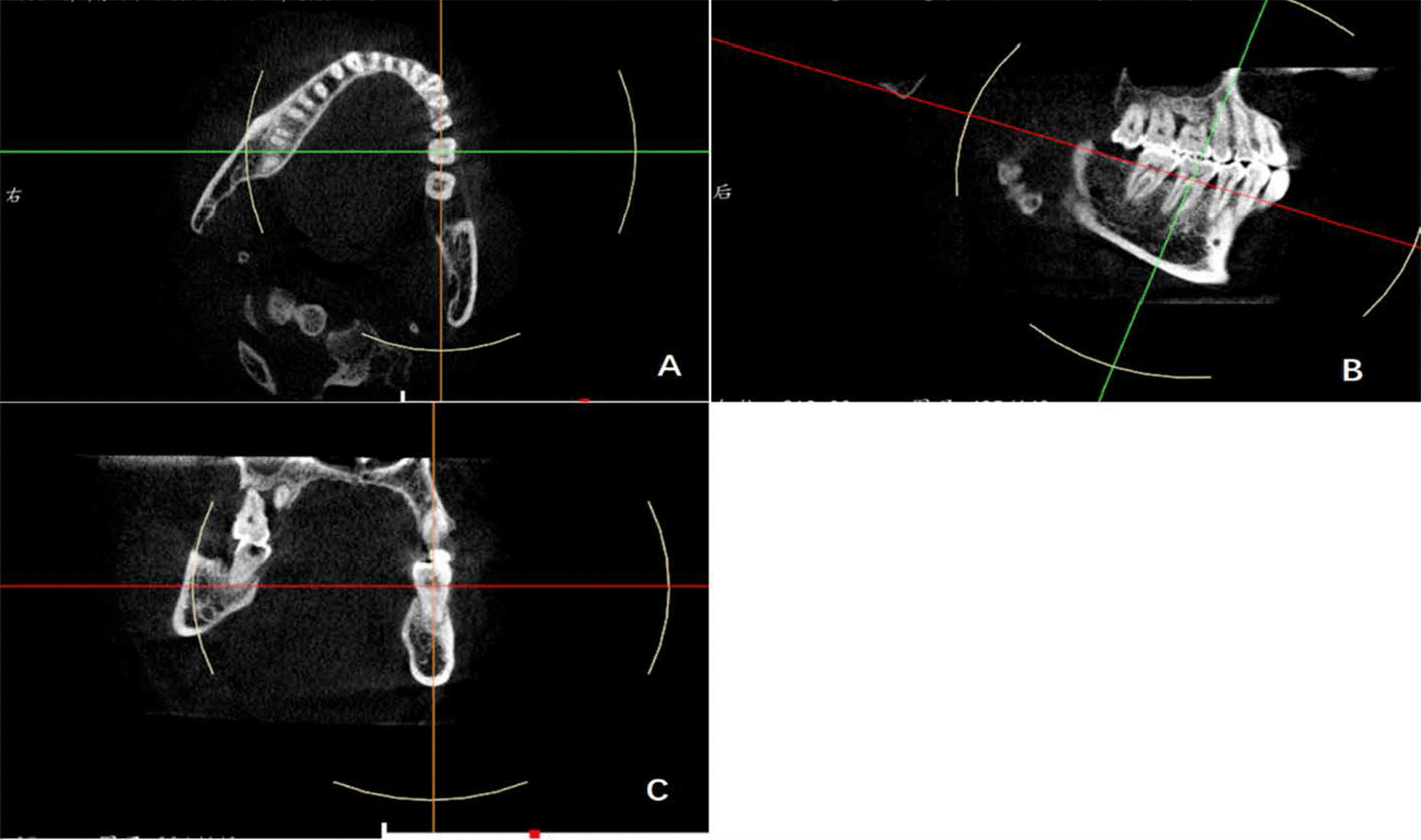
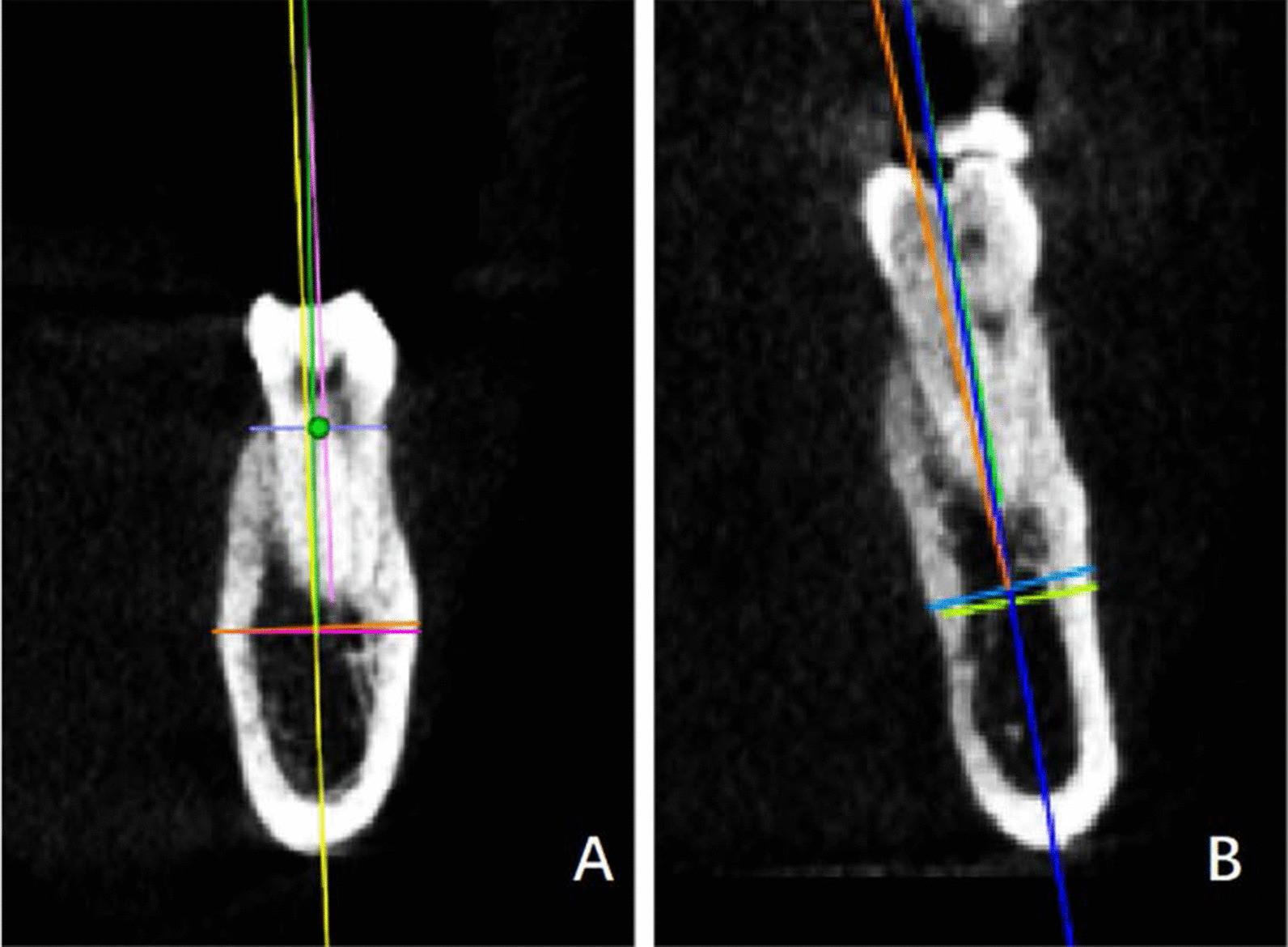
Methods: 201 CBCT data were reevaluated to measure height of the alveolar process (EF), width of the alveolar process (GH), width of the basal bone (IJ), the angle between the long axis of the first molar and the alveolar bone (∠a) and the angle between the long axis of the alveolar bone and basal bone (∠b). The angle and width were measured to determine the implant-prosthodontic classification of the morphology in the left lower first molar (36) and right lower first molar (46). All measurements were performed on the improved cross-sectional images.
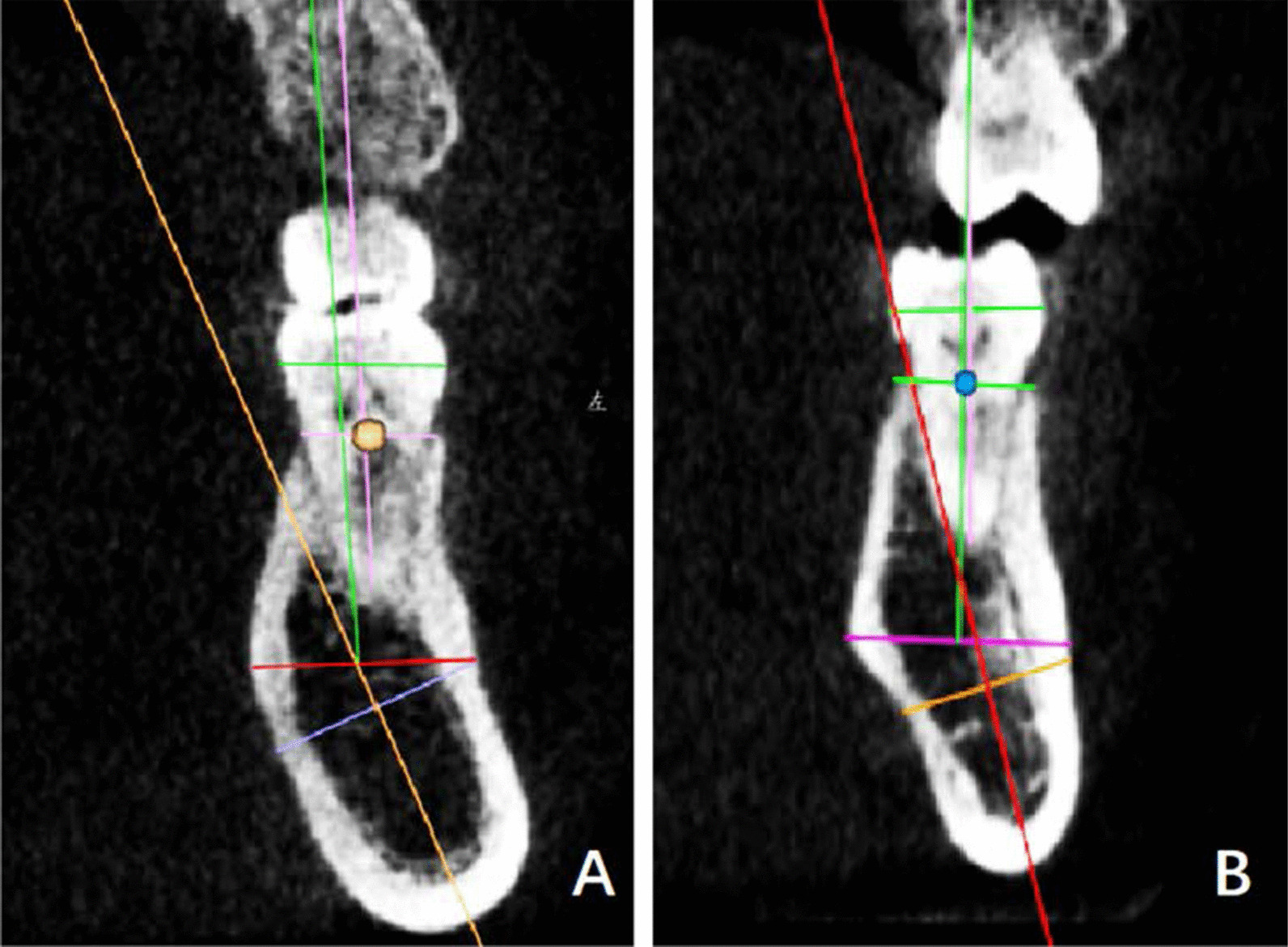
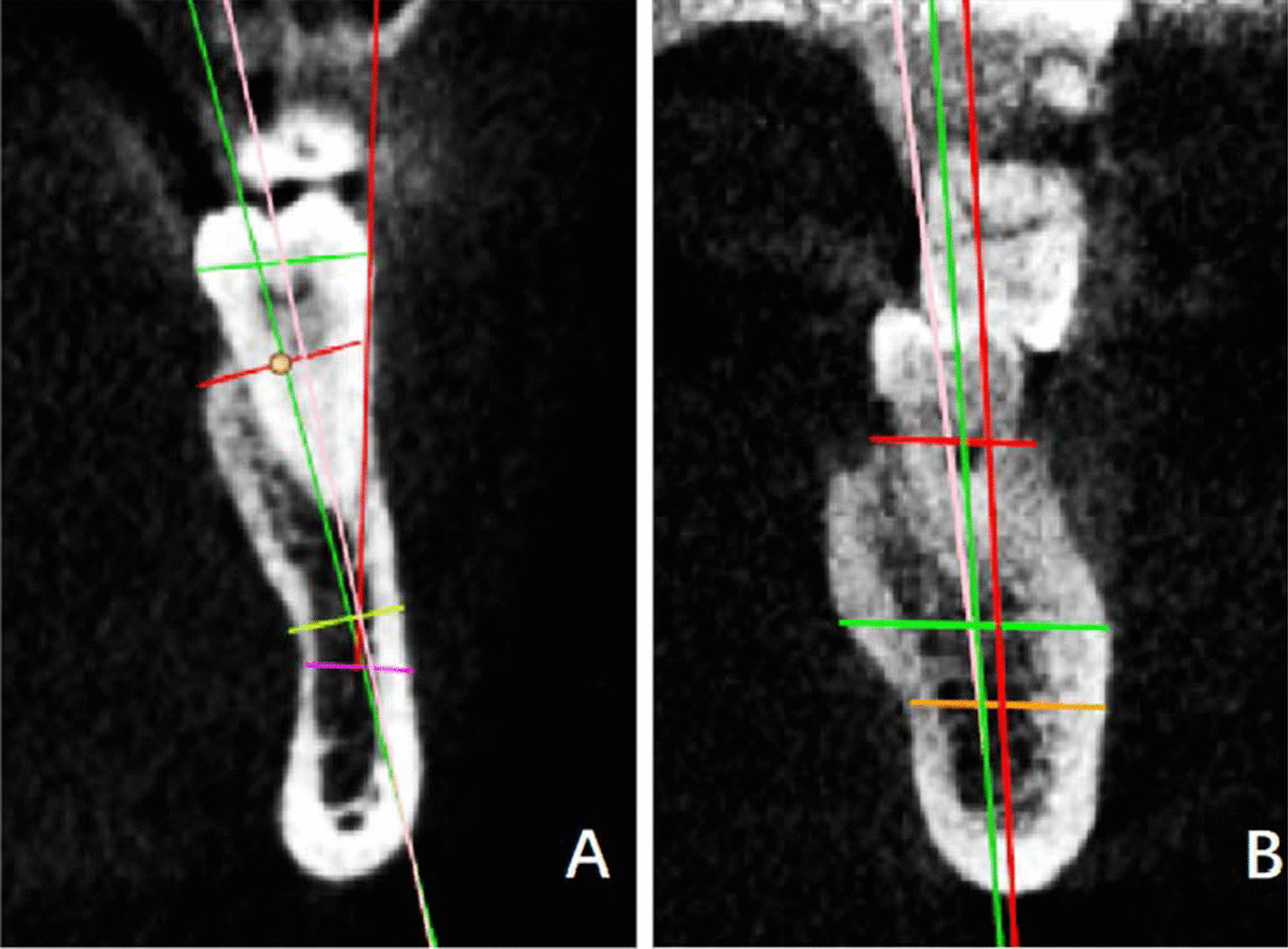
Results: EF, GH and IJ were measured as (10.83 ± 1.31) mm, (13.93 ± 2.00) mm and (12.68 ± 1.96) mm for 36, respectively; and (10.87 ± 1.24) mm, (13.86 ± 1.93) mm and (12.60 ± 1.90) mm for 46, respectively. No statistical significance was observed in EF, GH, IJ, ∠a and ∠b between 36 and 46 (all P > 0.05). The morphology was divided into three categories including the straight (68.7-69.2%), oblique (19.9-20.4%) and concave types (11%). Each type was consisted of two subcategories.
Conclusions: The proposed classification could provide evidence for appropriate selection and direction design of the mandibular molar implant in clinical. The concave type was the most difficult to implant with the highest risk of lingual perforation. The implant length, width, direction required more attention.
Keywords: Alveolar bone morphology; Cone-beam computed tomography; Dental implant; Mandibular molar.
© 2021. The Author(s).
Conflict of interest statement
The authors declared that they have no competing interests.
Figures





Similar articles
-
Relevant factors of posterior mandible lingual plate perforation during immediate implant placement: a virtual implant placement study using CBCT.BMC Oral Health. 2023 Feb 6;23(1):76. doi: 10.1186/s12903-022-02696-z. BMC Oral Health. 2023. PMID: 36747164 Free PMC article.
-
A CBCT-Based Comparative Study of Alveolar Bone Parameters and Implant Outcomes Among Patients Suffering the Mandibular First and Second Molar Defects.Ann Ital Chir. 2025;96(5):644-653. doi: 10.62713/aic.3951. Ann Ital Chir. 2025. PMID: 40375372
-
Finite element analysis of the angle range in trans-inferior alveolar nerve implantation at the mandibular second molar.BMC Oral Health. 2023 Nov 25;23(1):928. doi: 10.1186/s12903-023-03641-4. BMC Oral Health. 2023. PMID: 38007495 Free PMC article.
-
Evaluation of root canal morphology of human primary molars by using CBCT and comprehensive review of the literature.Acta Odontol Scand. 2016;74(4):250-8. doi: 10.3109/00016357.2015.1104721. Epub 2015 Nov 2. Acta Odontol Scand. 2016. PMID: 26523502 Review.
-
[Morphology of mandibular lingual concavities].Stomatologiia (Mosk). 2019;98(5):113-117. doi: 10.17116/stomat201998051113. Stomatologiia (Mosk). 2019. PMID: 31701940 Review. Russian.
Cited by
-
Relevant factors of posterior mandible lingual plate perforation during immediate implant placement: a virtual implant placement study using CBCT.BMC Oral Health. 2023 Feb 6;23(1):76. doi: 10.1186/s12903-022-02696-z. BMC Oral Health. 2023. PMID: 36747164 Free PMC article.
-
Evaluation of submandibular fossa depth and mandibular canal relationship with cone-beam computed tomography.BMC Oral Health. 2025 Apr 18;25(1):601. doi: 10.1186/s12903-025-05686-z. BMC Oral Health. 2025. PMID: 40251541 Free PMC article.
-
Quantitative and qualitative 3D analysis of mandibular lingual concavities: Implications for dental implant planning in the posterior mandible.Clin Exp Dent Res. 2024 Feb;10(1):e858. doi: 10.1002/cre2.858. Clin Exp Dent Res. 2024. PMID: 38345362 Free PMC article.
-
Effects of Crest Morphology on Lingual Concavity in Mandibular Molar Region: an Observational Study.J Oral Maxillofac Res. 2023 Mar 31;14(1):e3. doi: 10.5037/jomr.2023.14103. eCollection 2023 Jan-Mar. J Oral Maxillofac Res. 2023. PMID: 37180407 Free PMC article.
-
Anatomic Variations Important for Dental Implantation in the Mandible-A Systematic Review.Diagnostics (Basel). 2025 Jan 11;15(2):155. doi: 10.3390/diagnostics15020155. Diagnostics (Basel). 2025. PMID: 39857039 Free PMC article. Review.
References
-
- Misch CE. Occlusal considerations for implant-supported prostheses: implant-protective occlusion. In: Misch CE, editor. Dental implant prosthetics. 2. St Louis: Elsevier; 2015. pp. 874–912.
-
- Herranz-Aparicio J, Marques J, Almendros-Marqués N, et al. Retrospective study of the bone morphology in the posterior mandibular region. Evaluation of the prevalence and the degree of lingual concavity and their possible complications. Med Oral Patol Oral Cir Bucal. 2016;21:e731–e736. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
