

Shape-sensing robotic-assisted bronchoscopy for pulmonary nodules: initial multicenter experience using the Ion™ Endoluminal System
- PMID: 34656103
- PMCID: PMC8520632
- DOI: 10.1186/s12890-021-01693-2
Shape-sensing robotic-assisted bronchoscopy for pulmonary nodules: initial multicenter experience using the Ion™ Endoluminal System
Abstract
Background: Traditional bronchoscopy provides limited approach to peripheral nodules. Shape-sensing robotic-assisted bronchoscopy (SSRAB, Ion™ Endoluminal System) is a new tool for minimally invasive peripheral nodule biopsy. We sought to answer the research question: Does SSRAB facilitate sampling of pulmonary nodules during bronchoscopists' initial experience?
Methods: The lead-in stage of a multicenter, single-arm, prospective evaluation of the Ion Endoluminal System (PRECIsE) is described. Enrolled subjects ≥ 18 years old had recent computed tomography evidence of one or more solid or semi-solid pulmonary nodules ≥ 1.0 to ≤ 3.5 cm in greatest dimension and in any part of the lung. Subjects were followed at 10- and 30-days post-procedure. This stage provided investigators and staff their first human experience with the SSRAB system; safety and procedure outcomes were analyzed descriptively. Neither diagnostic yield nor sensitivity for malignancy were assessed in this stage. Categorical variables are summarized by percentage; continuous variables are summarized by median/interquartile range (IQR).
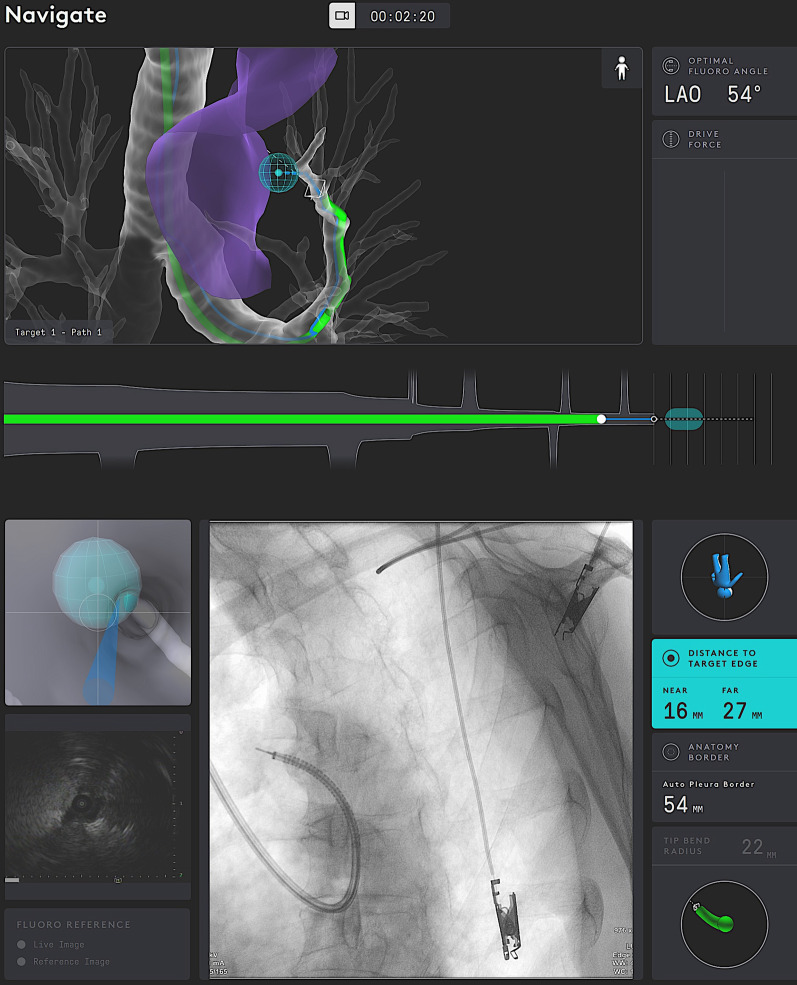
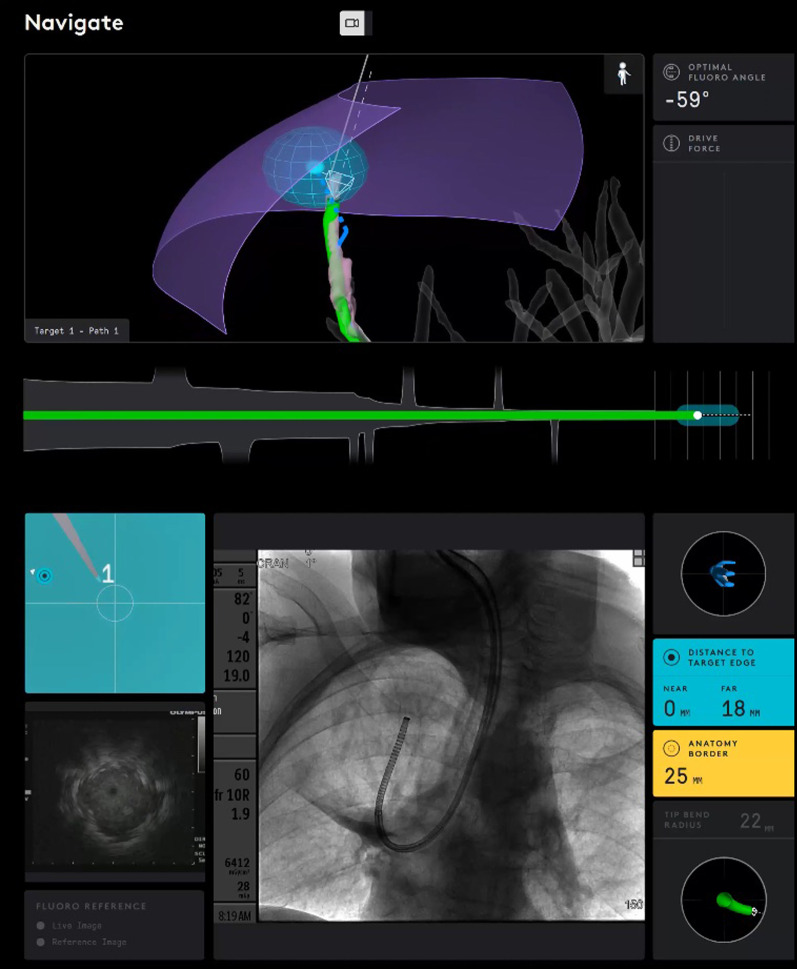
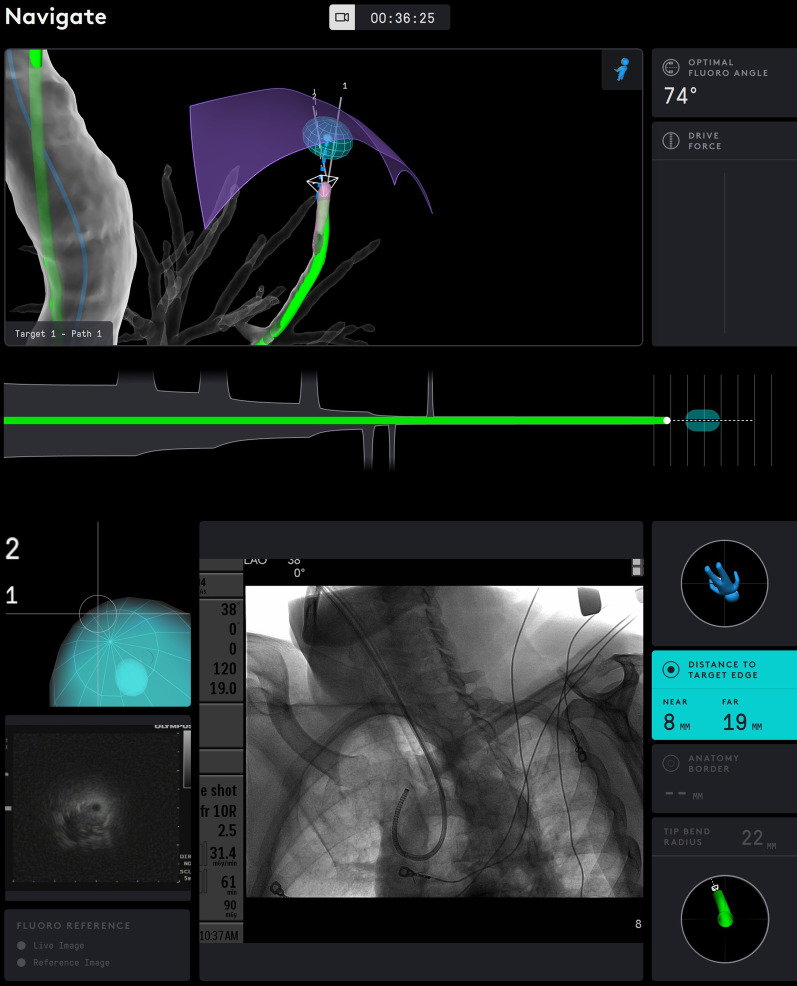
Results: Sixty subjects were enrolled across 6 hospitals; 67 nodules were targeted for biopsy. Median axial, coronal and sagittal diameters were < 18 mm with a largest cardinal diameter of 20.0 mm. Most nodules were extraluminal and distance from the outer edge of the nodule to the pleura or nearest fissure was 4.0 mm (IQR: 0.0, 15.0). Median bronchial generation count to the target location was 7.0 (IQR: 6.0, 8.0). Procedure duration (catheter-in to catheter-out) was 66.5 min (IQR: 50.0, 85.5). Distance from the catheter tip to the closest edge of the virtual nodule was 7.0 mm (IQR: 2.0, 12.0). Biopsy completion was 97.0%. No pneumothorax or airway bleeding of any grade was reported.
Conclusions: Bronchoscopists leveraged the Ion SSRAB's functionality to drive the catheter safely in close proximity of the virtual target and to obtain biopsies. This initial, multicenter experience is encouraging, suggesting that SSRAB may play a role in the management of pulmonary nodules. Clinical Trial Registration identifier and date NCT03893539; 28/03/2019.
Keywords: Biopsy; Bronchoscopy; Ion; Pulmonary nodules; Robotic assistance; Shape sensing.
© 2021. The Author(s).
Conflict of interest statement
MJS has received research and manuscript support from Intuitive Surgical and consulting fees and research support from Gongwin Biopharm. MAP has received consulting and speaker fees and research support from Johnson & Johnson, Medtronic, BodyVision, and Intuitive Surgical; research support from Philips; speaker fees and research support from Biodesix; consulting and speaker fees from AstraZeneca; speaker fees from Boeinger-Ingleheim; speaker fees and research support from United Therapeutics; speaker fees and research support from Actelion; research support from Inivata; consulting fees from Boston Scientific; consulting fees from OncoSec; consulting fees from Ambu; consulting fees and stock from HealthMyne. JSR has received research support and an educational grant from Intuitive Surgical. DEO has received research support, a research grant, and consulting fees from Intuitive Surgical. AM has received research support from Intuitive Surgical, consulting fees from Olympus America, and a research grant from Bronchus Medical. CK has received consulting fees and research support from Intuitive Surgical. RFC has received research support from Olympus, Concordia, Intuitive Surgical, and Siemens and consulting fees from Olympus, Siemens, Intuitive Surgical, Johnson & Johnson, and Bronx. MSP has received research support and educational consultant fees from Intuitive Surgical. JD-M has received research support from Intuitive Surgical. SF-B has received research support from Intuitive Surgical. EEF has received a research grant from Intuitive Surgical and consulting fees from Boston Scientific and Medtronic.
Figures




References
-
- Wahidi MW, Govert JA, Goudar RK, Gould MK, McCrory DC, and The American College of Chest Physicians. Evidence for the treatment of patients with pulmonary nodules: When is it lung cancer? ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132(3 Suppl):94s–107s. 10.1378/chest.07-1352. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
