

Dose reduction of the new generation biologics (IL-17 and IL-23 inhibitors) in psoriasis: study protocol for an international, pragmatic, multicenter, randomized, controlled, non-inferiority study-the BeNeBio study
- PMID: 34656148
- PMCID: PMC8520290
- DOI: 10.1186/s13063-021-05681-z
Dose reduction of the new generation biologics (IL-17 and IL-23 inhibitors) in psoriasis: study protocol for an international, pragmatic, multicenter, randomized, controlled, non-inferiority study-the BeNeBio study
Abstract
Background: Psoriasis is a chronic immune-mediated inflammatory skin disease for which biologics are effective treatments. Dose reduction (DR) of the first generation biologics seems a promising way for more efficient use of expensive biologics. A substantial part of patients on tumor necrosis factor (TNF)-alfa inhibitors and ustekinumab could successfully lower their dose, after following a tightly controlled DR strategy. The objective of this study is to assess whether controlled DR of interleukin (IL)-17 and IL-23 inhibitors in psoriasis patients with low disease activity is non-inferior (NI) to usual care (UC).
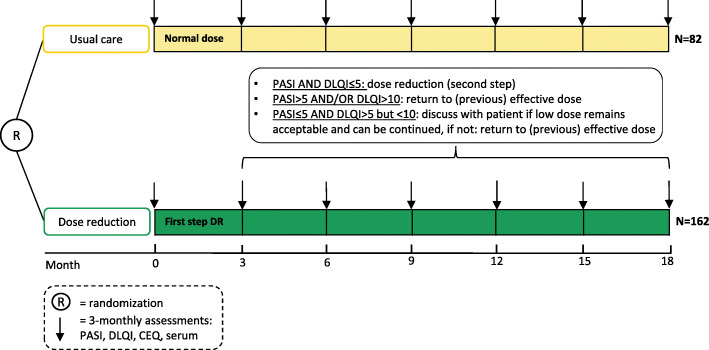
Methods: This is an international, prospective, multicenter, pragmatic, randomized, non-inferiority trial. A total of 244 patients with stable low disease activity (Psoriasis Area and Severity Index (PASI) ≤ 5) for at least 6 months and using secukinumab, ixekizumab, brodalumab, guselkumab, risankizumab, or tildrakizumab in the standard dose, together with stable low disease activity, defined as a PASI ≤ 5 and Dermatology Life Quality Index (DLQI) ≤ 5 at the moment of inclusion, will be randomized 2:1 to DR or UC. In the DR group, dosing intervals will be prolonged stepwise to achieve 66% and 50% of the original dose. Disease activity is monitored every 3 months by PASI and DLQI. In case of disease flare (i.e., PASI and/or DLQI increase), treatment is adjusted to the previous effective dose. The primary outcome is the incidence proportion of persistent flares (PASI > 5 for ≥ 3 months), which will be compared between arms. Secondary outcomes include proportion of patients with successful DR, (course of) PASI and DLQI, serious adverse events (SAEs), health-related quality of life, costs, and pharmacokinetic profile. Outcomes of DR will be compared to UC.
Discussion: With this study, we aim to assess whether DR of IL-17 and IL-23 inhibiting biologics can be achieved for psoriasis patients with low disease activity, without losing disease control. Reducing the dose may lead to more efficient use of biologics.
Trial registration: ClinicalTrials.gov NCT04340076 . Registered on April 9 2020.
Keywords: Biologics; Dose reduction; IL-17 inhibitors; IL-23 inhibitors; Non-inferiority; Psoriasis; Therapy.
© 2021. The Author(s).
Conflict of interest statement
LSS carries out clinical trials for Almirall, Janssen, and Novartis. All funding is not personal but goes to the independent Research Fund of the Department of Dermatology of the Radboud University Medical Centre Nijmegen, The Netherlands.
JMPAR carried out clinical trials for AbbVie, Celgene, and Janssen and has received speaking fees/attended advisory boards from AbbVie, Janssen, BMS, and Eli Lilly and reimbursement for attending a symposium from Janssen, Pfizer, Celgene, and AbbVie. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Center Nijmegen, the Netherlands.
LG has received speaker fee from AbbVie. All funding is not personal and goes to an independent research account of the department of dermatology of Ghent University Hospital, Ghent, Belgium.
LS has no competing interests.
WK has no competing interests.
EMGJJ has received research grants for the independent research fund of the department of dermatology of the Radboud university medical center Nijmegen, the Netherlands, from AbbVie, Pfizer, Novartis, Janssen Pharmaceuticals, and LEO Pharma and has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen Pharmaceutica, Novartis, Eli Lilly, Celgene, Leo Pharma, UCB, and Almirall. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Centre Nijmegen (Radboudumc), the Netherlands.
JLWL has received research grants from and/or acted as consultant/speaker for and has acted as consultant for AbbVie, Almirall, Amgen, Argenx, Eli Lilly, Janssen-Cilag, LEO Pharma, Novartis, Pfizer, and UCB. All funding is not personal and goes to an independent research account of the department of dermatology of Ghent University Hospital, Ghent, Belgium.
Figures
References
-
- Welsing PM, Bijl M, van Bodegraven AA, Lems WF, Prens E, Bijlsma JW. Cost effectiveness of biologicals: high costs are the other face of success. Ned Tijdschr Geneeskd. 2011;155(29):A3026. - PubMed
-
- Papp KA, Blauvelt A, Bukhalo M, Gooderham M, Krueger JG, Lacour JP, Menter A, Philipp S, Sofen H, Tyring S, Berner BR, Visvanathan S, Pamulapati C, Bennett N, Flack M, Scholl P, Padula SJ. Risankizumab versus ustekinumab for moderate-to-severe plaque psoriasis. N Engl J Med. 2017;376(16):1551–1560. doi: 10.1056/NEJMoa1607017. - DOI - PubMed
-
- Gordon KB, Blauvelt A, Papp KA, Langley RG, Luger T, Ohtsuki M, Reich K, Amato D, Ball SG, Braun DK, Cameron GS, Erickson J, Konrad RJ, Muram TM, Nickoloff BJ, Osuntokun OO, Secrest RJ, Zhao F, Mallbris L, Leonardi CL. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. N Engl J Med. 2016;375(4):345–356. doi: 10.1056/NEJMoa1512711. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
