

Video-assisted thoracic surgery sleeve resection and bronchoplasty using 3D imaging system: its safety and efficacy
- PMID: 34656152
- PMCID: PMC8520266
- DOI: 10.1186/s13019-021-01685-7
Video-assisted thoracic surgery sleeve resection and bronchoplasty using 3D imaging system: its safety and efficacy
Abstract
Background: Video-assisted thoracic surgery sleeve resection with bronchial anastomosis or bronchoplasty is a technically demanding procedure. Three-dimensional endoscopic surgery has been reported to be helpful in decreasing operation time and improving spatial perception with less surgical errors, but there have been rare reports about relatively difficult thoracoscopic procedures utilizing 3D thoracoscope. We performed this study to evaluate early clinical outcomes of thoracoscopic sleeve resection and bronchoplasty utilizing 3D thoracoscope.
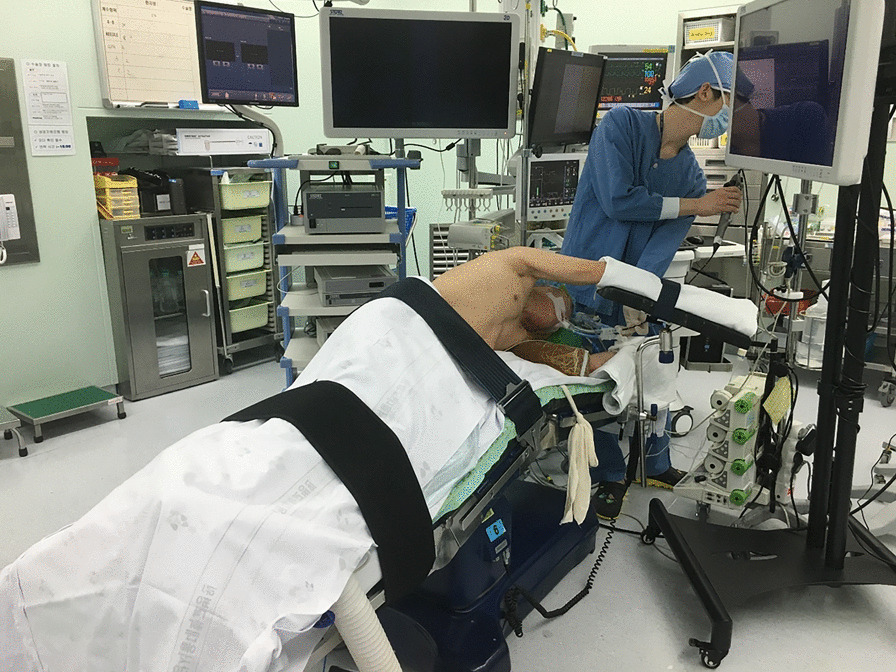
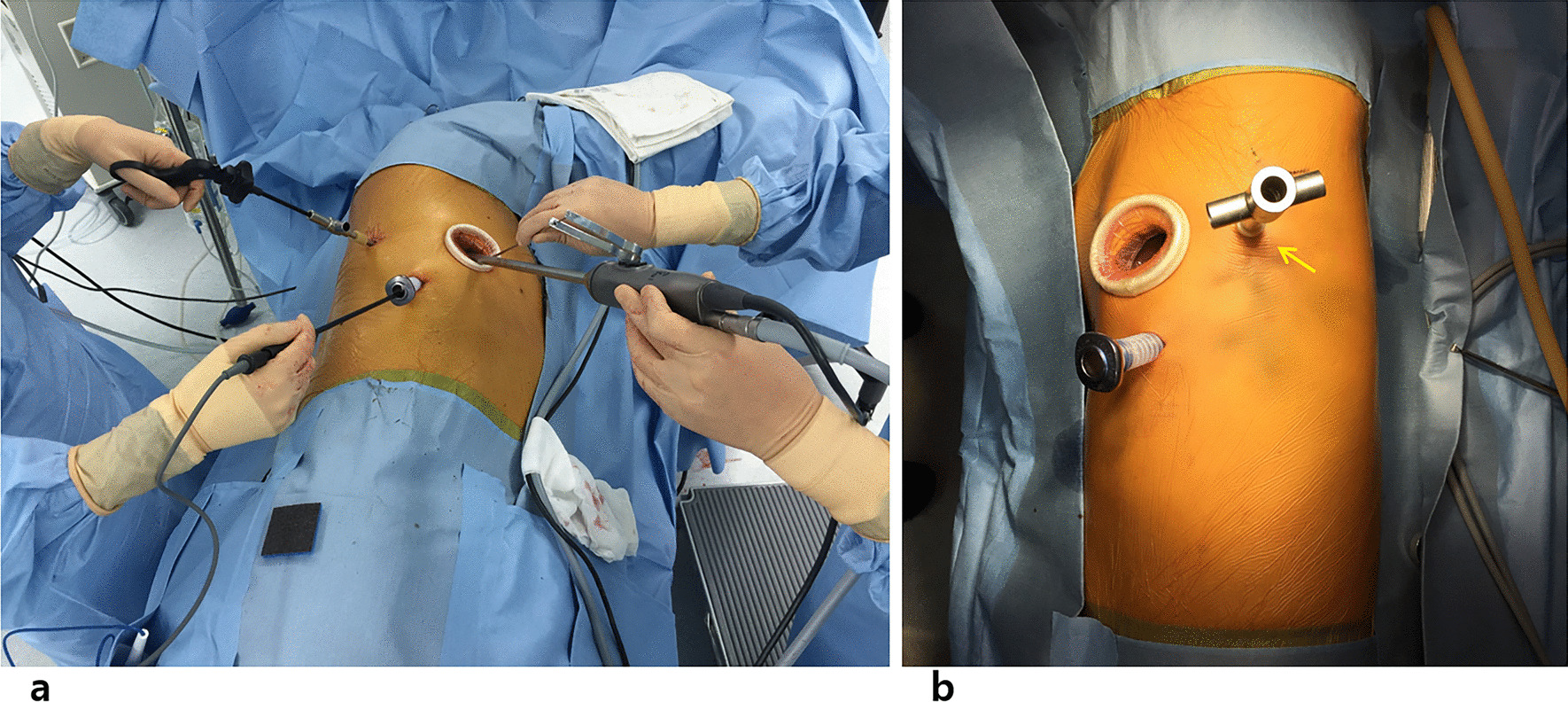
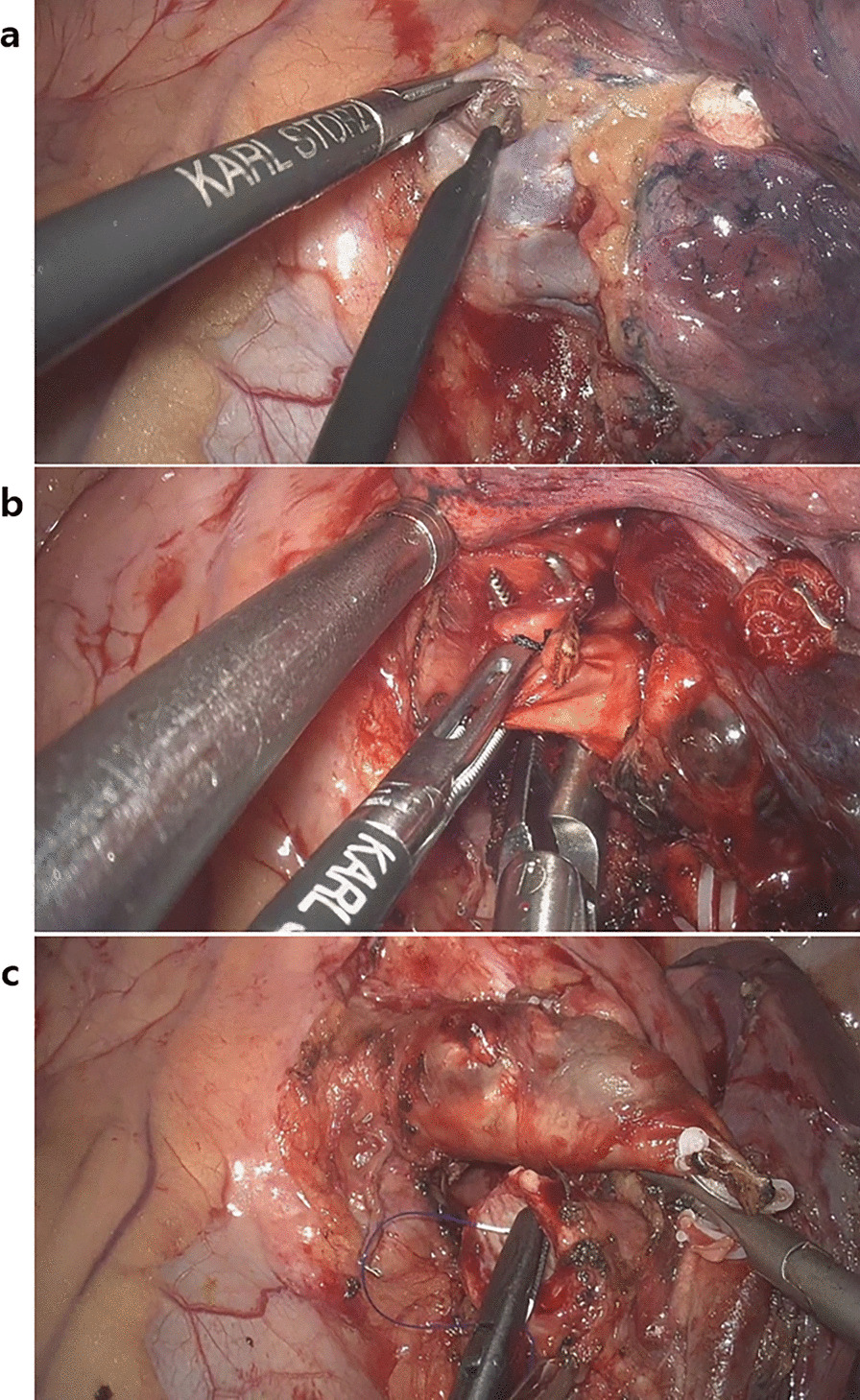
Methods: Data from a total of 36 patients who underwent thoracoscopic sleeve lobectomy or bronchoplasty at our institution from December 2015 to October 2017 were retrospectively reviewed. Three-port approach with one utility incision was used with a 10 mm, 30° three-dimensional thoracoscope. Twenty-three patients (81%) were male, and mean age was 65.9 ± 9.4 years. Fourteen patients (38.9%) underwent sleeve resection with bronchial anastomosis, 22 (61.1%) underwent wedge or simple bronchoplasty, and one patient received concomitant PA procedure. Bronchial anastomosis sites were not covered with viable tissue flaps.
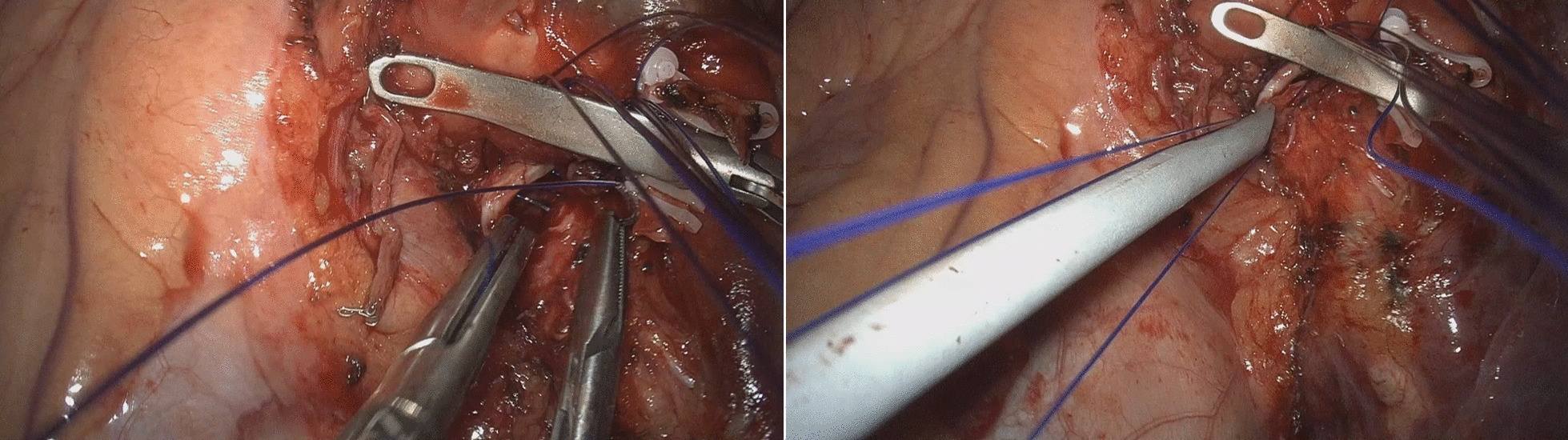
Results: There was no (0%) suture needle injury from spatial misperception during bronchoplasty or sleeve anastomosis. There was no (0%) operative mortality. The pathologic report revealed squamous cell carcinoma (63.9%), adenocarcinoma (19.4%), carcinoid (6.9%), adenosquamous carcinoma (3.4%), and sarcomatoid carcinoma (2.8%). One (2.8%) late mortality was due to systemic recurrence of sarcomatoid carcinoma. There was no (0.0%) anastomotic failure. The mean number of dissected lymph nodes were 27.4 ± 13.2, and mean operation time was 216.8 ± 60.0 min. Median postoperative 24-h drain amount was 315 mL. Median chest tube days and hospital days were 4 and 6, respectively. Two patients (5.6%) had complications greater than Clavien-Dindo grade II-one case of ARDS, and the other case of a delayed bronchopleural fistula.
Conclusions: Thoracoscopic sleeve resection and bronchoplasty utilizing HD 3D thoracoscope is a safe and effective procedure with excellent early clinical outcomes. Further investigation for long-term outcomes will be needed.
Keywords: Bronchi; Imaging; Lung cancer; Surgical anastomosis; Suture techniques; Three-dimensional; Video-assisted thoracic surgery.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Scott WJ, Allen MS, Darling G, Meyers B, Decker PA, Putnam JB, et al. Video-assisted thoracic surgery versus open lobectomy for lung cancer: a secondary analysis of data from the American College of Surgeons Oncology Group Z0030 randomized clinical trial. J Thorac Cardiovasc Surg. 2010;139(4):976–981. doi: 10.1016/j.jtcvs.2009.11.059. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
