

Predicting Survival in Repaired Tetralogy of Fallot: A Lesion-Specific and Personalized Approach
- PMID: 34656466
- PMCID: PMC8821017
- DOI: 10.1016/j.jcmg.2021.07.026
Predicting Survival in Repaired Tetralogy of Fallot: A Lesion-Specific and Personalized Approach
Abstract
Objectives: This study sought to identify patients with repaired tetralogy of Fallot (rTOF) at high risk of death and malignant ventricular arrhythmia (VA).
Background: To date there is no robust risk stratification scheme to predict outcomes in adults with rTOF.
Methods: Consecutive patients were prospectively recruited for late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) to define right and left ventricular (RV, LV) fibrosis in addition to proven risk markers.
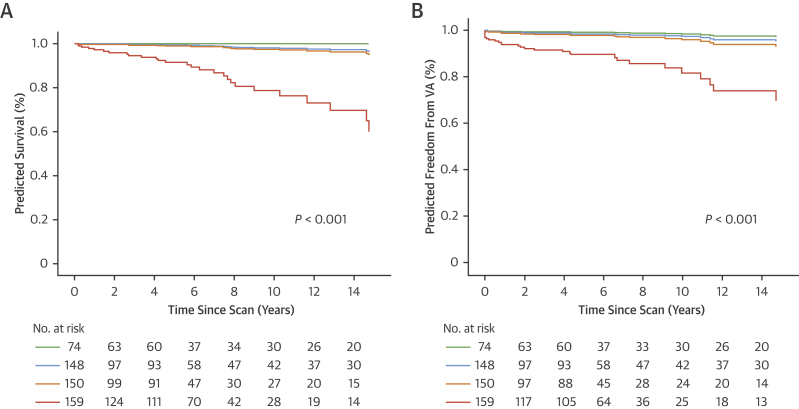
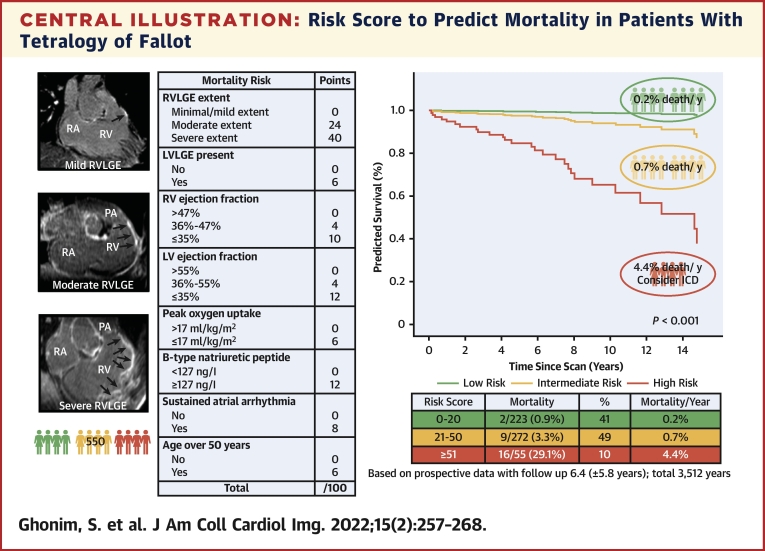
Results: The primary endpoint was all-cause mortality. Of the 550 patients (median age 32 years, 56% male), 27 died (mean follow-up 6.4 ± 5.8; total 3,512 years). Mortality was independently predicted by RVLGE extent, presence of LVLGE, RV ejection fraction ≤47%, LV ejection fraction ≤55%, B-type natriuretic peptide ≥127 ng/L, peak exercise oxygen uptake (V02) ≤17 mL/kg/min, prior sustained atrial arrhythmia, and age ≥50 years. The weighted scores for each of the preceding independent predictors differentiated a high-risk subgroup of patients with a 4.4%, annual risk of mortality (area under the curve [AUC]: 0.87; P < 0.001). The secondary endpoint (VA), a composite of life-threatening sustained ventricular tachycardia/resuscitated ventricular fibrillation/sudden cardiac death occurred in 29. Weighted scores that included several predictors of mortality and RV outflow tract akinetic length ≥55 mm and RV systolic pressure ≥47 mm Hg identified high-risk patients with a 3.7% annual risk of VA (AUC: 0.79; P < 0.001) RVLGE was heavily weighted in both risk scores caused by its strong relative prognostic value.
Conclusions: We present a score integrating multiple appropriately weighted risk factors to identify the subgroup of patients with rTOF who are at high annual risk of death who may benefit from targeted therapy.
Keywords: CMR; late gadolinium enhancement; risk stratification; sudden cardiac death; tetralogy of Fallot; ventricular tachycardia.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the British Heart Foundation (FS/11/38/28864), Drs Babu-Narayan and Heng were funded by the British Heart Foundation. Prof Dudley Pennell is a consultant to Siemens. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




Comment in
-
Getting Closer to Predicting SCD in TOF.JACC Cardiovasc Imaging. 2022 Feb;15(2):269-270. doi: 10.1016/j.jcmg.2021.09.022. Epub 2021 Nov 17. JACC Cardiovasc Imaging. 2022. PMID: 34801450 No abstract available.
-
Machine Learning to Predict Outcomes in Repaired Tetralogy of Fallot.JACC Cardiovasc Imaging. 2022 May;15(5):954-955. doi: 10.1016/j.jcmg.2022.01.020. JACC Cardiovasc Imaging. 2022. PMID: 35512963 No abstract available.
-
The Authors Reply.JACC Cardiovasc Imaging. 2022 May;15(5):955-956. doi: 10.1016/j.jcmg.2022.02.020. JACC Cardiovasc Imaging. 2022. PMID: 35512964 No abstract available.
References
-
- Gatzoulis M.A., Balaji S., Webber S.A., et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000;356:975–981. - PubMed
-
- Nollert G., Fischlein T., Bouterwek S., et al. Long-term survival in patients with repair of tetralogy of Fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol. 1997;30:1374–1383. - PubMed
-
- Silka M.J., Hardy B.G., Menashe V.D., et al. A population-based prospective evaluation of risk of sudden cardiac death after operation for common congenital heart defects. J Am Coll Cardiol. 1998;32:245–251. - PubMed
-
- Baumgartner H., De Backer J., Babu-Narayan S.V., et al. 2020 ESC Guidelines for the management of adult congenital heart disease. The Task Force for the management of adult congenital heart disease of the European Society of Cardiology (ESC) Eur Heart J. 2021;42(6):563–645. - PubMed
-
- Stout K.K., Daniels C.J., Aboulhosn J.A., et al. AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;139:698–800. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
