

A genetic risk score and diabetes predict development of alcohol-related cirrhosis in drinkers
- PMID: 34656649
- PMCID: PMC8803006
- DOI: 10.1016/j.jhep.2021.10.005
A genetic risk score and diabetes predict development of alcohol-related cirrhosis in drinkers
Erratum in
-
Corrigendum to: 'A genetic risk score and diabetes predict development of alcohol-related cirrhosis in drinkers' [J Hepatol 2022 (76) 275-282].J Hepatol. 2022 May;76(5):1244-1245. doi: 10.1016/j.jhep.2022.02.011. Epub 2022 Mar 11. J Hepatol. 2022. PMID: 35287983 No abstract available.
Abstract
Background & aims: Only a minority of excess alcohol drinkers develop cirrhosis. We developed and evaluated risk stratification scores to identify those at highest risk.
Methods: Three cohorts (GenomALC-1: n = 1,690, GenomALC-2: n = 3,037, UK Biobank: relevant n = 6,898) with a history of heavy alcohol consumption (≥80 g/day (men), ≥50 g/day (women), for ≥10 years) were included. Cases were participants with alcohol-related cirrhosis. Controls had a history of similar alcohol consumption but no evidence of liver disease. Risk scores were computed from up to 8 genetic loci identified previously as associated with alcohol-related cirrhosis and 3 clinical risk factors. Score performance for the stratification of alcohol-related cirrhosis risk was assessed and compared across the alcohol-related liver disease spectrum, including hepatocellular carcinoma (HCC).
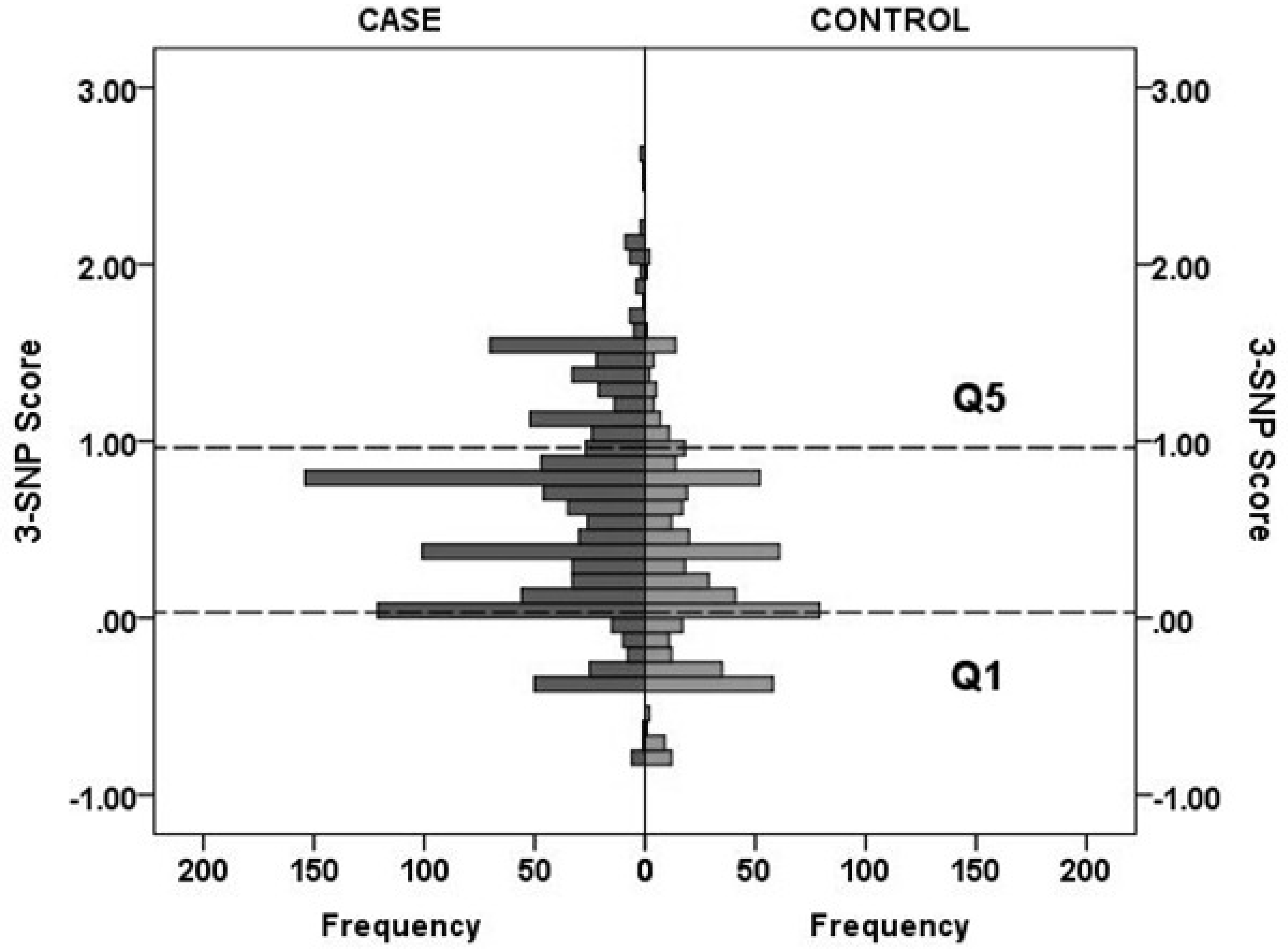
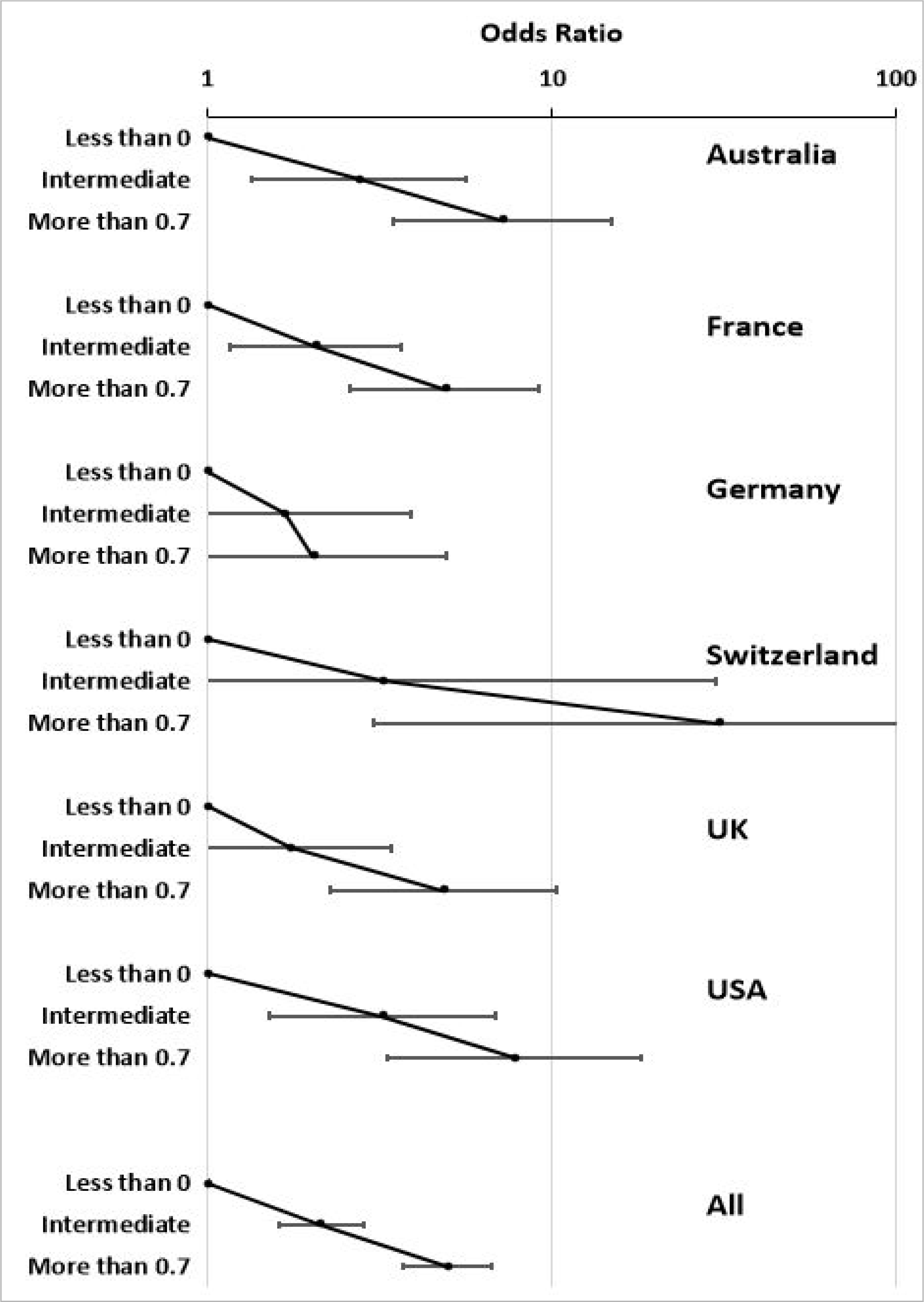
Results: A combination of 3 single nucleotide polymorphisms (SNPs) (PNPLA3:rs738409, SUGP1-TM6SF2:rs10401969, HSD17B13:rs6834314) and diabetes status best discriminated cirrhosis risk. The odds ratios (ORs) and (95% CIs) between the lowest (Q1) and highest (Q5) score quintiles of the 3-SNP score, based on independent allelic effect size estimates, were 5.99 (4.18-8.60) (GenomALC-1), 2.81 (2.03-3.89) (GenomALC-2), and 3.10 (2.32-4.14) (UK Biobank). Patients with diabetes and high risk scores had ORs of 14.7 (7.69-28.1) (GenomALC-1) and 17.1 (11.3-25.7) (UK Biobank) compared to those without diabetes and with low risk scores. Patients with cirrhosis and HCC had significantly higher mean risk scores than patients with cirrhosis alone (0.76 ± 0.06 vs. 0.61 ± 0.02, p = 0.007). Score performance was not significantly enhanced by information on additional genetic risk variants, body mass index or coffee consumption.
Conclusions: A risk score based on 3 genetic risk variants and diabetes status enables the stratification of heavy drinkers based on their risk of cirrhosis, allowing for the provision of earlier preventative interventions.
Lay summary: Excessive chronic drinking leads to cirrhosis in some people, but so far there is no way to identify those at high risk of developing this debilitating disease. We developed a genetic risk score that can identify patients at high risk. The risk of cirrhosis is increased >10-fold with just two risk factors - diabetes and a high genetic risk score. Risk assessment using this test could enable the early and personalised management of this disease in high-risk patients.
Keywords: Hepatocellular carcinoma; chronic alcohol use; coffee; genome-wide association; risk stratification; single nucleotide polymorphism.
Copyright © 2021 European Association for the Study of the Liver. All rights reserved.
Conflict of interest statement
Conflict of interest NPC has a number of consulting agreements with and research grants from the pharmaceutical industry but they are not significantly or directly related to this paper. MP receives research funding from various organisations including the MRC and NIHR. He has also received partnership funding for the following: MRC Clinical Pharmacology Training Scheme (co-funded by MRC and Roche, UCB, Eli Lilly and Novartis); a PhD studentship jointly funded by EPSRC and Astra Zeneca; and grant funding from Vistagen Therapeutics. He has also unrestricted educational grant support for the UK Pharmacogenetics and Stratified Medicine Network from Bristol-Myers Squibb and UCB. He has developed an HLA genotyping panel with MC Diagnostics, but does not benefit financially from this. He is part of the IMI Consortium ARDAT (www.ardat.org). None of these funding sources were deployed in the undertaking of this study. TRM has conducted clinical research with AbbVie, Genfit, Gilead, and Merck but none of these are related to this manuscript. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Comment in
-
Genetic factors in alcohol-related cirrhosis.Nat Rev Gastroenterol Hepatol. 2021 Dec;18(12):832. doi: 10.1038/s41575-021-00545-y. Nat Rev Gastroenterol Hepatol. 2021. PMID: 34725493 No abstract available.
-
External validation of a genetic risk score that predicts development of alcohol-related cirrhosis.J Hepatol. 2022 Dec;77(6):1720-1721. doi: 10.1016/j.jhep.2022.06.006. Epub 2022 Jun 14. J Hepatol. 2022. PMID: 35710038 No abstract available.
-
Reply to: "External validation of a genetic risk score that predicts development of alcohol-related cirrhosis".J Hepatol. 2022 Dec;77(6):1721-1722. doi: 10.1016/j.jhep.2022.08.024. Epub 2022 Aug 31. J Hepatol. 2022. PMID: 36055430 No abstract available.
References
-
- Hasin DS, Stinson FS, Ogburn E, Grant BF: Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 2007, 64:830–42. 10.1001/archpsyc.64.7.830. - DOI - PubMed
-
- Pequignot G, Tuyns AJ, Berta JL: Ascitic cirrhosis in relation to alcohol consumption. IntJEpidemiol 1978, 7:113–20. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AA026917/AA/NIAAA NIH HHS/United States
- NIHR 200153/DH_/Department of Health/United Kingdom
- U01 AA021886/AA/NIAAA NIH HHS/United States
- U24 AG021886/AG/NIA NIH HHS/United States
- MR/R014019/1/MRC_/Medical Research Council/United Kingdom
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- MR/L006758/1/MRC_/Medical Research Council/United Kingdom
- U01 AA018389/AA/NIAAA NIH HHS/United States
- R01 AA025208/AA/NIAAA NIH HHS/United States
- R28 AA012725/AA/NIAAA NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- I01 CX000361/CX/CSRD VA/United States
- R01 AA018389/AA/NIAAA NIH HHS/United States
