

Preclinical models versus clinical renal ischemia reperfusion injury: A systematic review based on metabolic signatures
- PMID: 34657378
- PMCID: PMC9298342
- DOI: 10.1111/ajt.16868
Preclinical models versus clinical renal ischemia reperfusion injury: A systematic review based on metabolic signatures
Abstract
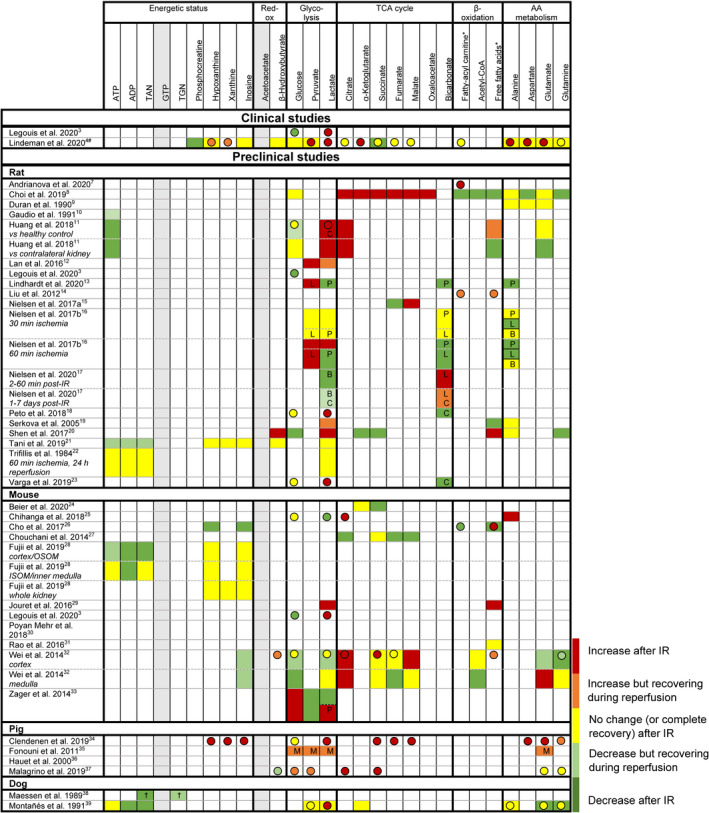
Despite decennia of research and numerous successful interventions in the preclinical setting, renal ischemia reperfusion (IR) injury remains a major problem in clinical practice, pointing toward a translational gap. Recently, two clinical studies on renal IR injury (manifested either as acute kidney injury or as delayed graft function) identified metabolic derailment as a key driver of renal IR injury. It was reasoned that these unambiguous metabolic findings enable direct alignment of clinical with preclinical data, thereby providing the opportunity to elaborate potential translational hurdles between preclinical research and the clinical context. A systematic review of studies that reported metabolic data in the context of renal IR was performed according to the PRISMA guidelines. The search (December 2020) identified 35 heterogeneous preclinical studies. The applied methodologies were compared, and metabolic outcomes were semi-quantified and aligned with the clinical data. This review identifies profound methodological challenges, such as the definition of IR injury, the follow-up time, and sampling techniques, as well as shortcomings in the reported metabolic information. In light of these findings, recommendations are provided in order to improve the translatability of preclinical models of renal IR injury.
Keywords: animal models; delayed graft function; ischemia reperfusion injury; kidney failure / injury; kidney transplantation / nephrology; metabolomics; translational research / science.
© 2021 The Authors. American Journal of Transplantation published by Wiley Periodicals LLC on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
