

Effects and tolerability of exercise therapy modality on cardiorespiratory fitness in lung cancer: a randomized controlled trial
- PMID: 34658160
- PMCID: PMC8718021
- DOI: 10.1002/jcsm.12828
Effects and tolerability of exercise therapy modality on cardiorespiratory fitness in lung cancer: a randomized controlled trial
Abstract
Background: Poor cardiorespiratory fitness (CRF) is a cardinal feature of post-treatment primary lung cancer. The most effective exercise therapy regimen to improve CRF has not been determined.
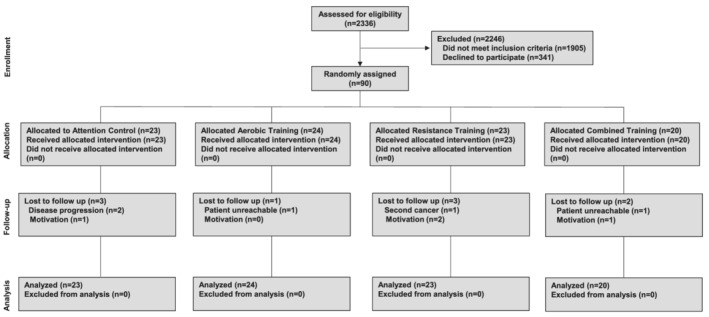
Methods: In this parallel-group factorial randomized controlled trial, lung cancer survivors with poor CRF (below age-sex sedentary values) were randomly allocated to receive 48 consecutive supervised sessions thrice weekly of (i) aerobic training (AT)-cycle ergometry at 55% to >95% of peak oxygen consumption (VO2 peak); (ii) resistance training (RT)-lower and upper extremity exercises at 50-85% of maximal strength; (iii) combination training (CT)-AT plus RT; or (iv) stretching attention control (AC) for 16 weeks. The primary endpoint was change in CRF (VO2 peak, mL O2 ·kg-1 ·min-1 ). Secondary endpoints were body composition, muscle strength, patient-reported outcomes, tolerability (relative dose intensity of exercise), and safety. Analysis of covariance determined change in primary and secondary endpoints from baseline to post-intervention (Week 17) with adjustment for baseline values of the endpoint and other relevant clinical covariates.
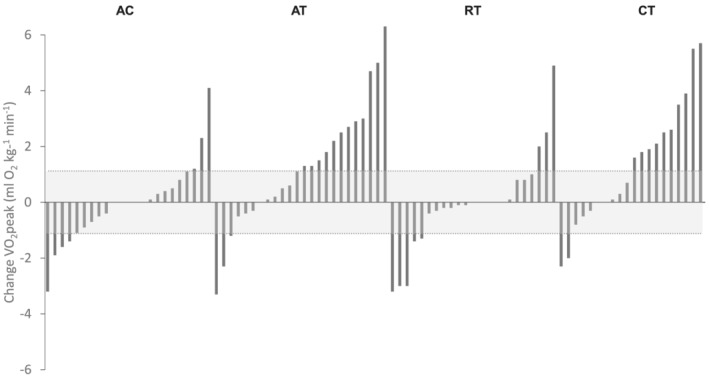
Results: Ninety patients (65 ± 9 years; 66% female) were randomized (AT, n = 24; RT, n = 23; CT, n = 20; and AC, n = 23) of the planned n = 160. No serious adverse events were observed. For the overall cohort, the lost-to-follow-up rate was 10%. Mean attendance was ≥75% in all groups. In intention-to-treat analysis, VO2 peak increased 1.1 mL O2 ·kg-1 ·min-1 [95% confidence interval (CI): 0.0, 2.2, P = 0.04] and 1.4 mL O2 ·kg-1 ·min-1 (95% CI: 0.2, 2.5, P = 0.02) in AT and CT, respectively, compared with AC. There was no difference in VO2 peak change between RT and AC (-0.1 mL O2 ·kg-1 ·min-1 , 95% CI: -1.2, 1.0, P = 0.88). Favourable improvements in maximal strength and body composition were observed in RT and CT groups compared with AT and AC groups (Ps < 0.05). No between-group changes were observed for any patient-reported outcomes. Relative dose intensity of exercise was lower in RT and CT compared with AT (Ps < 0.05).
Conclusions: In the context of a smaller than planned sample size, AT and CT significantly improved VO2 peak in lung cancer survivors; however, the tolerability-to-benefit ratio was superior for AT and hence may be the preferred modality to target impaired CRF in post-treatment lung cancer survivors.
Trial registration: ClinicalTrials.gov NCT01068210.
Keywords: Aerobic training; Cancer survivorship; Combination training; Exercise capacity; Resistance training.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
L.W.J. has stock ownership in Pacylex, Inc. Other authors report no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30. - PubMed
-
- Nezu K, Kushibe K, Tojo T, Takahama M, Kitamura S. Recovery and limitation of exercise capacity after lung resection for lung cancer. Chest 1998;113:1511–1516. - PubMed
-
- Brunelli A, Pompili C, Salati M, Refai M, Berardi R, Mazzanti P, et al. Preoperative maximum oxygen consumption is associated with prognosis after pulmonary resection in stage I non‐small cell lung cancer. Ann Thorac Surg 2014;98:238–242. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
