

Hybrid Left Heart Bypass Circuit for Repair of the Descending Aorta in an 8-kg Williams Syndrome Patient
- PMID: 34658410
- PMCID: PMC8499637
- DOI: 10.1182/ject-2100022
Hybrid Left Heart Bypass Circuit for Repair of the Descending Aorta in an 8-kg Williams Syndrome Patient
Abstract
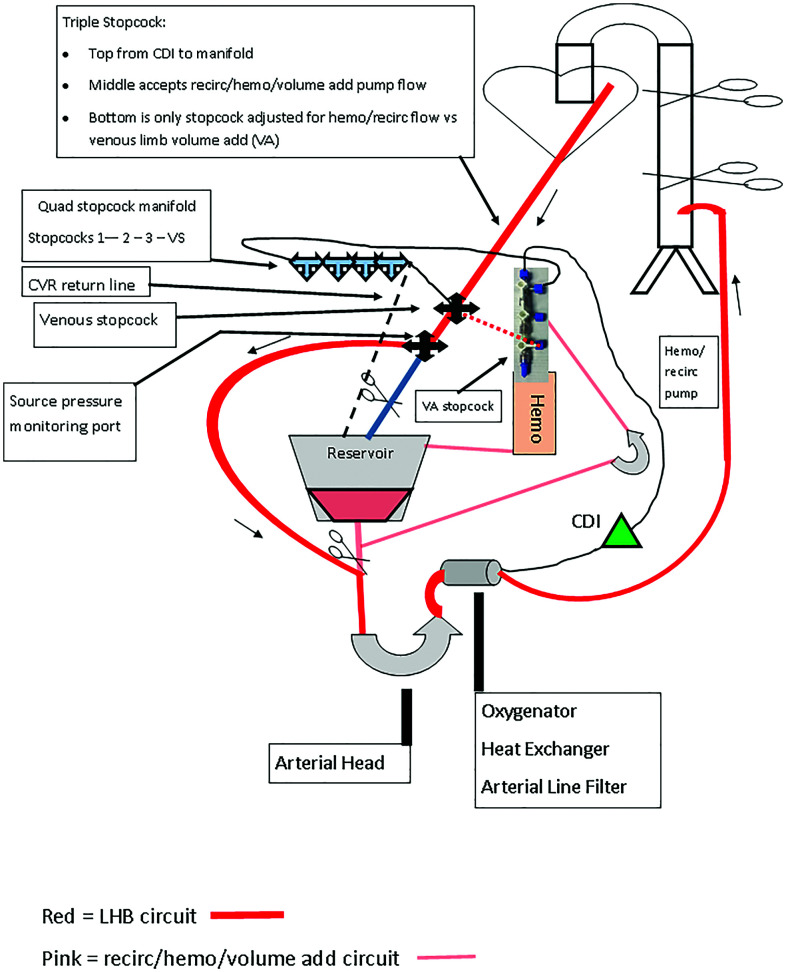
A 1-year old male patient with Williams syndrome and multiple prior interventions presented for surgical repair of his descending aorta (DA) through a left thoracotomy. Concerns for significant bleeding and spinal cord protection led the care team to consider a left heart bypass (LHB) circuit with options for pump sucker use, heat exchange capacity, and the possibility of converting to traditional cardiopulmonary bypass (CPB). A traditional CPB circuit with a roller-head arterial pump was assembled with a bypass line around the cardiotomy venous reservoir (CVR). Excluding the CVR with this line allowed for a closed LHB circuit. A second pump head was integrated to both recirculate the CVR volume and to serve as a means for controlled volume administration to the closed LHB circuit. Pump sucker return directed to the CVR could easily be transfused back to the patient. The patient was placed on the hybrid LHB circuit and cooled to 32°C. DA clamps were placed. Upper body dynamic blood pressure was managed for a target mean of 50 mmHg, the left atrial pressure (LAP) was maintained in the 5-7 mmHg range, and the nonpulsatile lower body blood pressure was targeted at 40-50 mmHg. Cerebral near-infrared spectroscopy (NIRS) helped guide volume and pressure management. The surgeons placed two long-segment patches on the DA, moving clamps as needed. The patient was rewarmed and separated from the hybrid LHB circuit after 82 minutes. Closed circuit LHB can be provided with a roller-head hybrid circuit incorporating an oxygenator for gas exchange, central cooling and warming, and arterial line filtration along with a CVR for pump sucker use and controlled transfusion to the patient.
Keywords: METEOR circuit; Williams syndrome; hybrid left heart bypass circuit; left heart bypass; pediatric; pump suckers.
© Copyright 2021 AMSECT.
Figures
Similar articles
-
The application of modular multifunctional left heart bypass circuit system integrated with ultrafiltration in thoracoabdominal aortic aneurysm repair.Front Cardiovasc Med. 2022 Sep 21;9:944287. doi: 10.3389/fcvm.2022.944287. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36211541 Free PMC article.
-
The BICIRCUIT system: innovative perfusional options for surgical treatment of the thoracic aorta.Ann Thorac Surg. 2005 Feb;79(2):678-80; discussion 680-1. doi: 10.1016/j.athoracsur.2003.11.060. Ann Thorac Surg. 2005. PMID: 15680858 Clinical Trial.
-
Limitations using the vacuum-assist venous drainage technique during cardiopulmonary bypass procedures.J Extra Corpor Technol. 2003 Sep;35(3):207-11. J Extra Corpor Technol. 2003. PMID: 14653422
-
Recent Advances in Pediatric Cardiopulmonary Bypass.Semin Cardiothorac Vasc Anesth. 2014 Jun;18(2):153-60. doi: 10.1177/1089253214525279. Semin Cardiothorac Vasc Anesth. 2014. PMID: 24876230 Review.
-
The Society of Thoracic Surgeons, The Society of Cardiovascular Anesthesiologists, and The American Society of ExtraCorporeal Technology: Clinical Practice Guidelines for Cardiopulmonary Bypass--Temperature Management During Cardiopulmonary Bypass.J Cardiothorac Vasc Anesth. 2015 Aug;29(4):1104-13. doi: 10.1053/j.jvca.2015.07.011. J Cardiothorac Vasc Anesth. 2015. PMID: 26279227 Review.
Cited by
-
The application of modular multifunctional left heart bypass circuit system integrated with ultrafiltration in thoracoabdominal aortic aneurysm repair.Front Cardiovasc Med. 2022 Sep 21;9:944287. doi: 10.3389/fcvm.2022.944287. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36211541 Free PMC article.
-
Modified Circuit for Left-Sided Heart Bypass in Thoracoabdominal Surgery.Ann Thorac Surg Short Rep. 2023 Sep 13;2(1):21-24. doi: 10.1016/j.atssr.2023.09.003. eCollection 2024 Mar. Ann Thorac Surg Short Rep. 2023. PMID: 39790259 Free PMC article.
References
-
- Coselli JS. The use of left heart bypass in the repair of thoracoabdominal aortic aneurysms: current techniques and results. Semin Thorac Cardiovasc Surg. 2003;15:326–32. - PubMed
-
- Kouchoukos NT, Wareing TH, Izumoto H, et al. . Elective hypothermia and cardiopulmonary bypass and circulatory arrest for spinal cord protection during operations on the thoracoabdominal aorta. J Thorac Cardiovasc Surg. 1990;99:659–64. - PubMed
-
- Wahlgren CM, Blohmé L, Günther A, et al. . Outcomes of left heart bypass versus circulatory arrest in elective open surgical descending and thoraco-abdominal aortic repair. Eur J Vasc Endovasc Surg. 2017;53:672–8. - PubMed
-
- Papadimas E, Tan YK, Qi Q, et al. . Left heart bypass versus circulatory arrest for open repair of thoracoabdominal aortic pathologies. ANZ J Surg. 2020;90:2434–40. - PubMed
-
- Said SM, Burkhart HM, Dearani JA, et al. . Ascending-to-descending aortic bypass: a simple solution to a complex problem. Ann Thorac Surg. 2014;97:2041–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials