

Hyperinflammatory Immune Response and COVID-19: A Double Edged Sword
- PMID: 34659238
- PMCID: PMC8515020
- DOI: 10.3389/fimmu.2021.742941
Hyperinflammatory Immune Response and COVID-19: A Double Edged Sword
Abstract
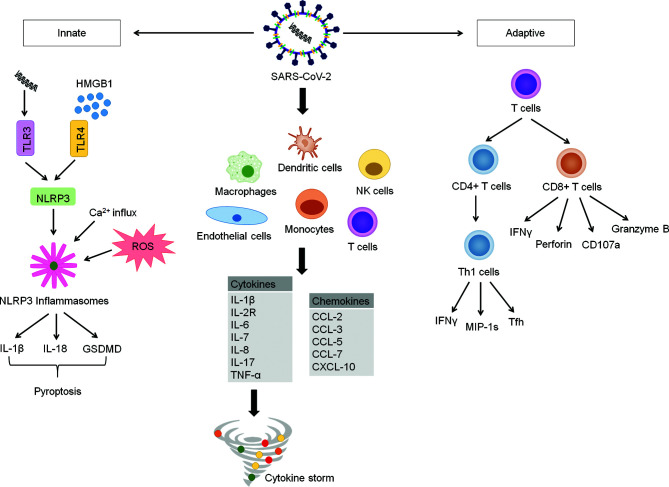
The coronavirus disease-19 (COVID-19) elicited by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused devastating health, economic and social impact worldwide. Its clinical spectrum ranges from asymptomatic to respiratory failure and multi-organ failure or death. The pathogenesis of SARS-CoV-2 infection is attributed to a complex interplay between virus and host immune response. It involves activation of multiple inflammatory pathways leading to hyperinflammation and cytokine storm, resulting in tissue damage, acute respiratory distress syndrome (ARDS) and multi-organ failure. Accumulating evidence has raised concern over the long-term health effects of COVID-19. Importantly, the neuroinvasive potential of SARS-CoV-2 may have devastating consequences in the brain. This review provides a conceptual framework on how the virus tricks the host immune system to induce infection and cause severe disease. We also explore the key differences between mild and severe COVID-19 and its short- and long-term effects, particularly on the human brain.
Keywords: COVID-19; SARS-CoV-2; adaptive immune response; cytokine storm; hyperinflammation; immunopathogenesis; innate immune response.
Copyright © 2021 Tan, Komarasamy and RMT Balasubramaniam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . WHO Coronavirus Disease (COVID-19) Dashboard (2021). Available at: https://covid19.who.int/. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous