

Lemmel's syndrome due to giant periampullary diverticulum: report of a case
- PMID: 34659600
- PMCID: PMC8502835
- DOI: 10.1016/j.radcr.2021.08.068
Lemmel's syndrome due to giant periampullary diverticulum: report of a case
Abstract
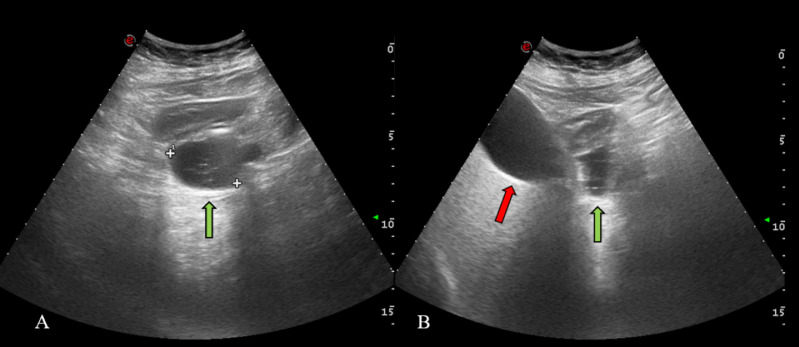
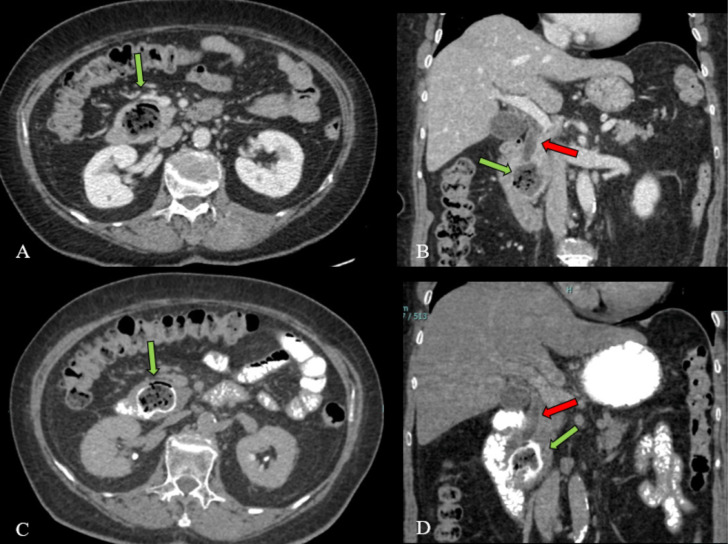
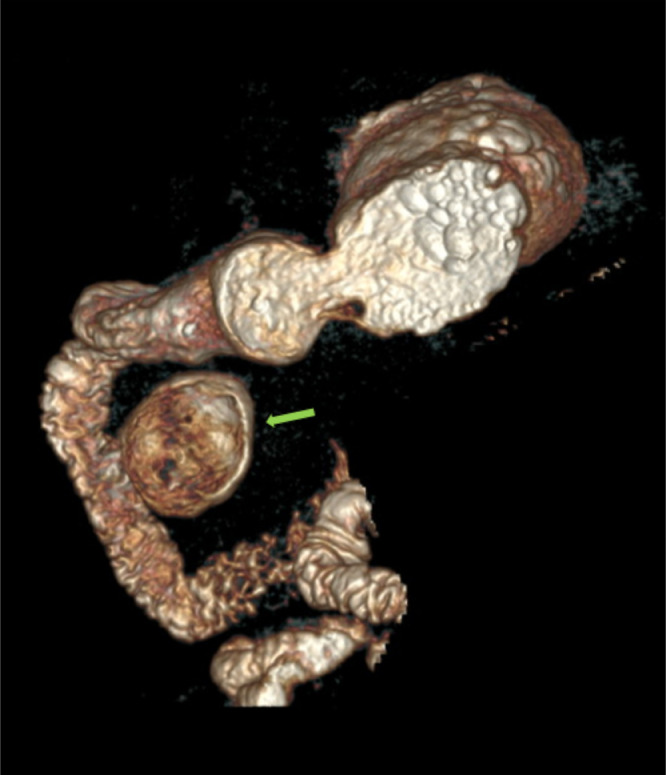
Lemmel's syndrome is a rare cause of obstructive jaundice in the absence of stones or tumors, commonly due to periampullary duodenal diverticulum (PAD). CT scan with the oral and intravenous administration of iodinated contrast media, was crucial to exclude the presence of stones or tumours, but esophagogastroduodenoscopy (EGD) confirms the diagnosis. We report a case of a 72 -year-old woman affected by Lemmel's syndrome secondary to a giant PAD, suffering from right upper abdominal quadrant pain and pancreaticobiliary disease. Subsequently we proceed to analyse the pathogenesis of PAD, and later to discuss pitfalls, tips and tricks useful to make a correct diagnosis, in order to achieve an accurate management.
Keywords: Cholangitis; Lemmel's syndrome; Pancreaticobiliary disease; Pancreatitis; Periampullary duodenal diverticulum.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures

References
-
- Vitturi N, Simoni F, De Stefano F, Orlando R, Lirussi F, Realdi G. Paravaterian diverticula presenting as acute cholangitis in two very elderly patients. J Gastrointestin Liver Dis. 2010;19(2):220–221. - PubMed
-
- Pimparkar BD. In: Gastroenterology. 3rd (Ed) Bockus Henry L, editor. WB Saunders Co; Philadelphia: 1976. Diverticulosis of the small intestine In; pp. 437–458. (Ed)
-
- Cheshire NJ, Diverticula Glezer G. In: Maingoats Abdominal operation. 10th (Ed) Zinner MJ, Schwartz SI, Ellis H, editors. Prentice Hall International Ince (UK) Limited; London: 2021. volvulus, superior mesenteric artery syndrome and foreign bodies. In. (Ed) 916-2.
-
- Mahajan Sanjay, Rajesh Kashyap, K Chandel, Mokta Jatinder, S Minhas. (2004). Duodenal diverticulum: Review of literature. Ind J Surge. 2004;66:140–145. Num 366.
Publication types
LinkOut - more resources
Full Text Sources
