

Remote Training of Functional Endoscopic Sinus Surgery With Advanced Manufactured 3D Sinus Models and a Telemedicine System
- PMID: 34660685
- PMCID: PMC8517106
- DOI: 10.3389/fsurg.2021.746837
Remote Training of Functional Endoscopic Sinus Surgery With Advanced Manufactured 3D Sinus Models and a Telemedicine System
Abstract
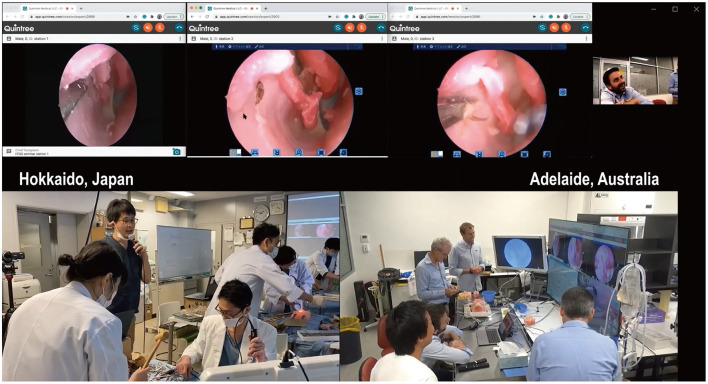
Objective: Traditionally, cadaveric courses have been an important tool in surgical education for Functional Endoscopic Sinus Surgery (FESS). The recent COVID-19 pandemic, however, has had a significant global impact on such courses due to its travel restrictions, social distancing regulations, and infection risk. Here, we report the world-first remote (Functional Endoscopic Sinus Surgery) FESS training course between Japan and Australia, utilizing novel 3D-printed sinus models. We examined the feasibility and educational effect of the course conducted entirely remotely with encrypted telemedicine software. Methods: Three otolaryngologists in Hokkaido, Japan, were trained to perform frontal sinus dissections on novel 3D sinus models of increasing difficulty, by two rhinologists located in Adelaide, South Australia. The advanced manufactured sinus models were 3D printed from the Computed tomography (CT) scans of patients with chronic rhinosinusitis. Using Zoom and the Quintree telemedicine platform, the surgeons in Adelaide first lectured the Japanese surgeons on the Building Block Concept for a three Dimensional understanding of the frontal recess. They in real time directly supervised the surgeons as they planned and then performed the frontal sinus dissections. The Japanese surgeons were asked to complete a questionnaire pertaining to their experience and the time taken to perform the frontal dissection was recorded. The course was streamed to over 200 otolaryngologists worldwide. Results: All dissectors completed five frontal sinusotomies. The time to identify the frontal sinus drainage pathway (FSDP) significantly reduced from 1,292 ± 672 to 321 ± 267 s (p = 0.02), despite an increase in the difficulty of the frontal recess anatomy. Image analysis revealed the volume of FSDP was improved (2.36 ± 0.00 to 9.70 ± 1.49 ml, p = 0.014). Questionnaires showed the course's general benefit was 95.47 ± 5.13 in dissectors and 89.24 ± 15.75 in audiences. Conclusion: The combination of telemedicine software, web-conferencing technology, standardized 3D sinus models, and expert supervision, provides excellent training outcomes for surgeons in circumstances when classical surgical workshops cannot be realized.
Keywords: 3D printer; building block concept; frontal sinusotomy; functional endoscopic sinus surgery (FESS); social distancing regulation; surgical training.
Copyright © 2021 Suzuki, Vyskocil, Ogi, Matoba, Nakamaru, Homma, Wormald and Psaltis.
Conflict of interest statement
MS: receiving royalties from Igakushoin. PW: consultant for Fusetec, Neilmed and receiving royalties from Medtronic, Fusetec, and Integra. Shareholder for Chitogel. AP: consultant for Fusetec, Medtronic, Tissium, and ENT technologies. Shareholder for Chitogel and Speakers Bureau for Sequiris. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources