

Automated subcortical volume estimation from 2D MRI in epilepsy and implications for clinical trials
- PMID: 34661698
- PMCID: PMC9005416
- DOI: 10.1007/s00234-021-02811-x
Automated subcortical volume estimation from 2D MRI in epilepsy and implications for clinical trials
Abstract
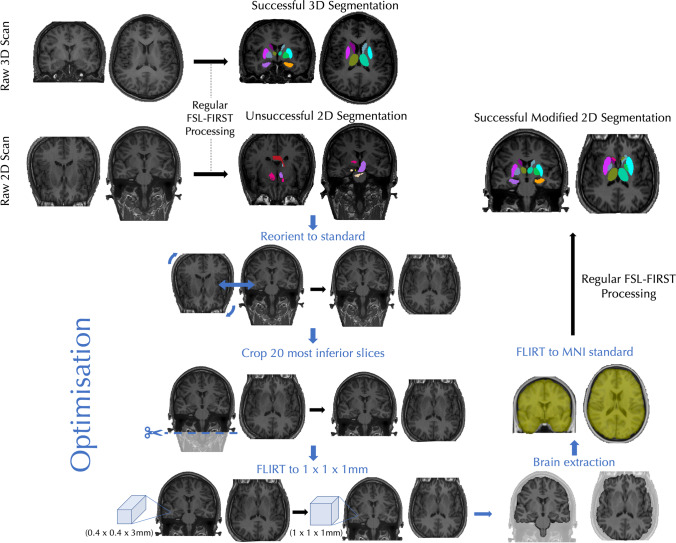
Purpose: Most techniques used for automatic segmentation of subcortical brain regions are developed for three-dimensional (3D) MR images. MRIs obtained in non-specialist hospitals may be non-isotropic and two-dimensional (2D). Automatic segmentation of 2D images may be challenging and represents a lost opportunity to perform quantitative image analysis. We determine the performance of a modified subcortical segmentation technique applied to 2D images in patients with idiopathic generalised epilepsy (IGE).
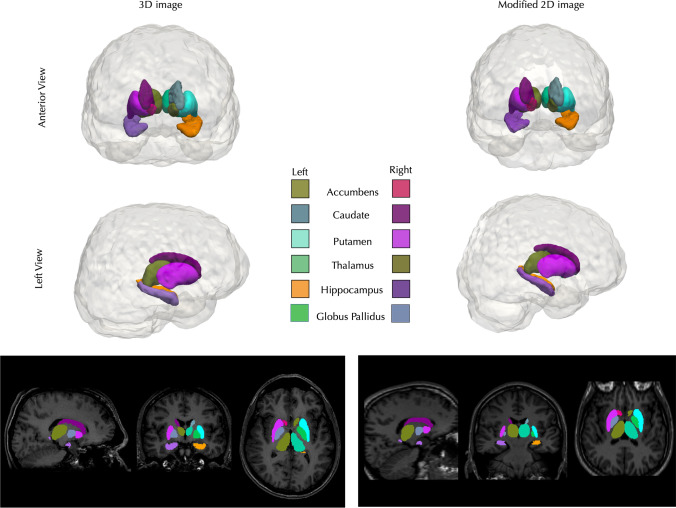
Methods: Volume estimates were derived from 2D (0.4 × 0.4 × 3 mm) and 3D (1 × 1x1mm) T1-weighted acquisitions in 31 patients with IGE and 39 healthy controls. 2D image segmentation was performed using a modified FSL FIRST (FMRIB Integrated Registration and Segmentation Tool) pipeline requiring additional image reorientation, cropping, interpolation and brain extraction prior to conventional FIRST segmentation. Consistency between segmentations was assessed using Dice coefficients and volumes across both approaches were compared between patients and controls. The influence of slice thickness on consistency was further assessed using 2D images with slice thickness increased to 6 mm.
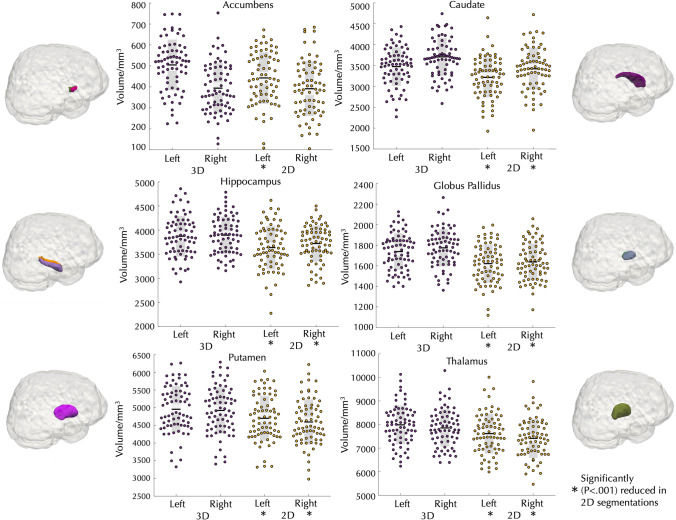
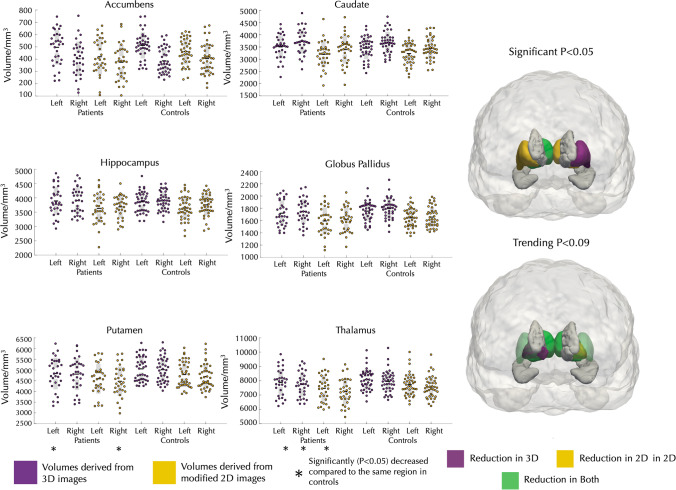
Results: All average Dice coefficients showed excellent agreement between 2 and 3D images across subcortical structures (0.86-0.96). Most 2D volumes were consistently slightly lower compared to 3D volumes. 2D images with increased slice thickness showed lower agreement with 3D images with lower Dice coefficients (0.55-0.83). Significant volume reduction of the left and right thalamus and putamen was observed in patients relative to controls across 2D and 3D images.
Conclusion: Automated subcortical volume estimation of 2D images with a resolution of 0.4 × 0.4x3mm using a modified FIRST pipeline is consistent with volumes derived from 3D images, although this consistency decreases with an increased slice thickness. Thalamic and putamen atrophy has previously been reported in patients with IGE. Automated subcortical volume estimation from 2D images is feasible and most reliable at using in-plane acquisitions greater than 1 mm x 1 mm and provides an opportunity to perform quantitative image analysis studies in clinical trials.
Keywords: Automatic segmentation; Epilepsy; Subcortical; Two-dimensional segmentation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
