

The Applicability of Commonly Used Severity of Illness Scores to Tropical Infections in Australia
- PMID: 34662860
- PMCID: PMC8733535
- DOI: 10.4269/ajtmh.21-0615
The Applicability of Commonly Used Severity of Illness Scores to Tropical Infections in Australia
Abstract
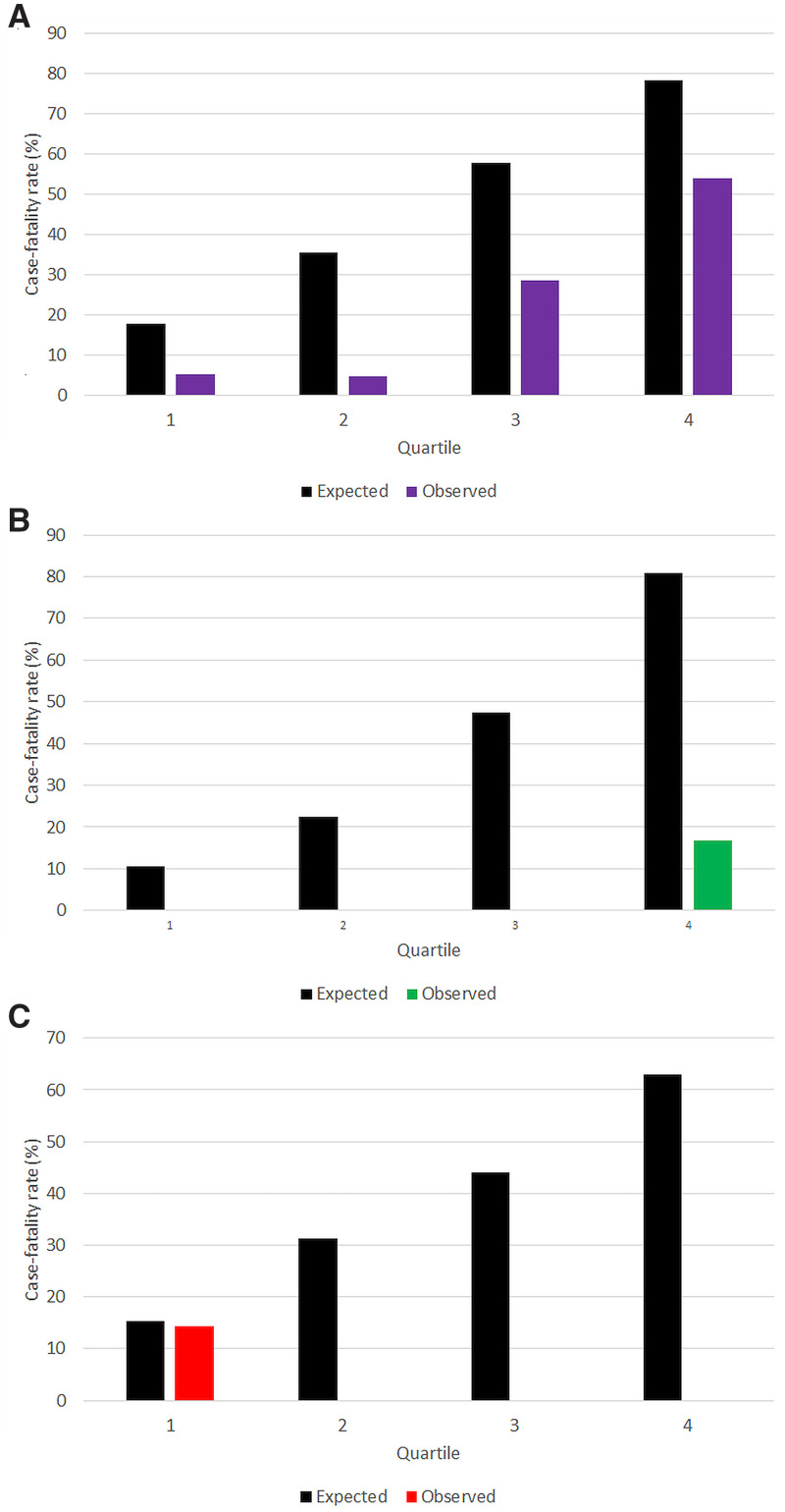
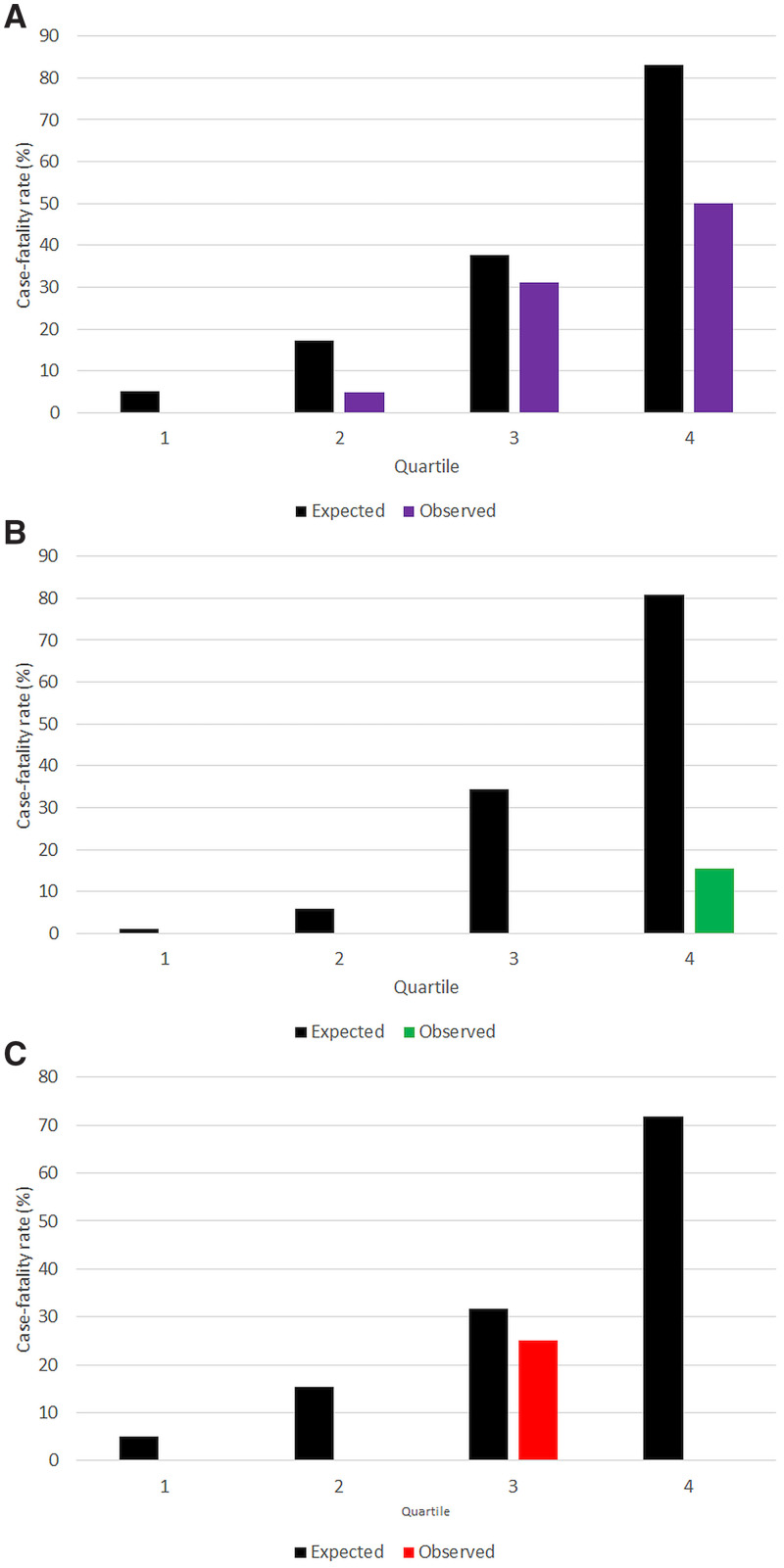
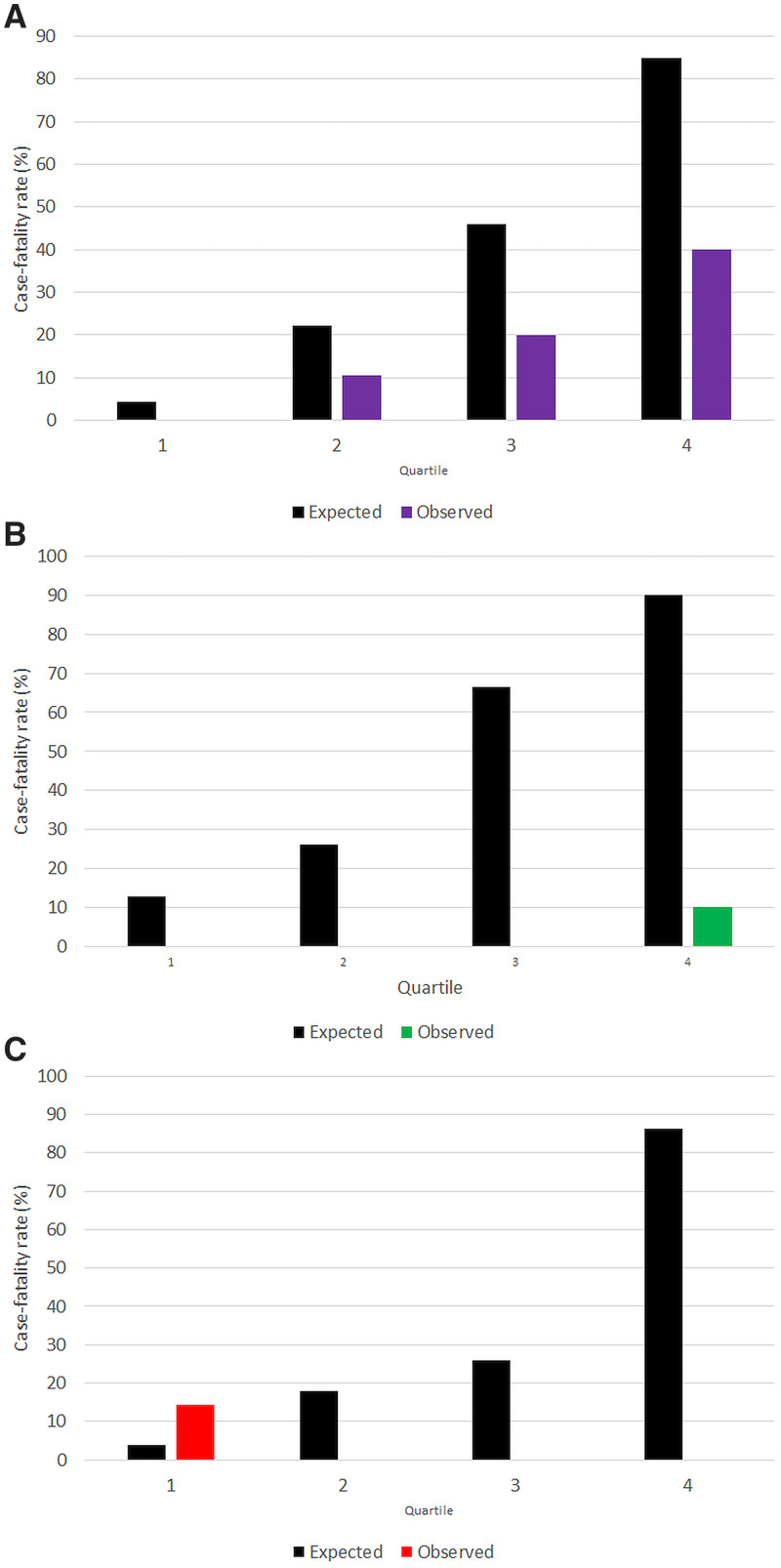
Many patients with leptospirosis, melioidosis, and rickettsial infection require intensive care unit (ICU) admission in tropical Australia every year. The multi-organ dysfunction associated with these infections results in significantly elevated severity of illness (SOI) scores. However, the accuracy of these SOI scores in predicting death from these tropical infections is incompletely defined. This retrospective study was performed at Cairns Hospital, a tertiary-referral hospital in tropical Australia. All patients admitted to ICU with laboratory-confirmed leptospirosis, melioidosis, and rickettsial disease between January 1, 1999 and June 30, 2020, were eligible for the study. The ability of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, Simplified Acute Physiology Scores (SAPS) II, and Sequential Organ Failure Assessment (SOFA) scores to predict death before ICU discharge was evaluated. Overall, 18 (12.1%) of the 149 included patients died: 15/74 (20.3%) with melioidosis, 2/54 (3.7%) with leptospirosis and 1/21 (4.8%) with rickettsial disease. However, the APACHE II, APACHE III, SAPS II, and SOFA scores significantly overestimated the case-fatality rate of all the infections; the disparity between the predicted and observed mortality was most marked in the cases of leptospirosis and rickettsial disease. Commonly used SOI scores significantly overestimate the case-fatality rate of melioidosis, leptospirosis, and rickettsial infections in Australian ICU patients. This may be at least partly explained by the unique pathophysiology of these infections, particularly leptospirosis and rickettsial disease. However, SOI scores may still be useful in facilitating the comparison of disease severity in clinical trials that examine patients with these pathogens.
Figures



References
-
- Kaukonen K-M, Bailey M, Suzuki S, Pilcher D, Bellomo R, 2014. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 311: 1308–1316. - PubMed
-
- McGloughlin S, Richards GA, Nor MBM, Prayag S, Baker T, Amin P, 2018. Sepsis in tropical regions: report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. J Crit Care 46: 115–118. - PubMed
-
- Davis JS, Cheng AC, McMillan M, Humphrey AB, Stephens DP, Anstey NM, 2011. Sepsis in the tropical top end of Australia’s Northern Territory: disease burden and impact on Indigenous Australians. Med J Aust 194: 519–524. - PubMed
-
- Sundararajan V, Macisaac CM, Presneill JJ, Cade JF, Visvanathan K, 2005. Epidemiology of sepsis in Victoria, Australia. Crit Care Med 33: 71–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
