

Causes and Outcomes of Admission and Investigation of Tuberculosis in Adults with Advanced HIV in South African Hospitals: Data from the TB Fast Track Trial
- PMID: 34662866
- PMCID: PMC8641325
- DOI: 10.4269/ajtmh.21-0133
Causes and Outcomes of Admission and Investigation of Tuberculosis in Adults with Advanced HIV in South African Hospitals: Data from the TB Fast Track Trial
Abstract
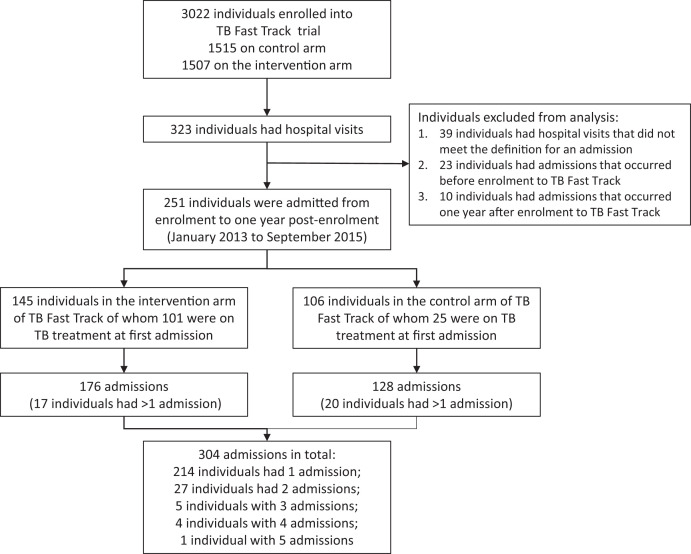
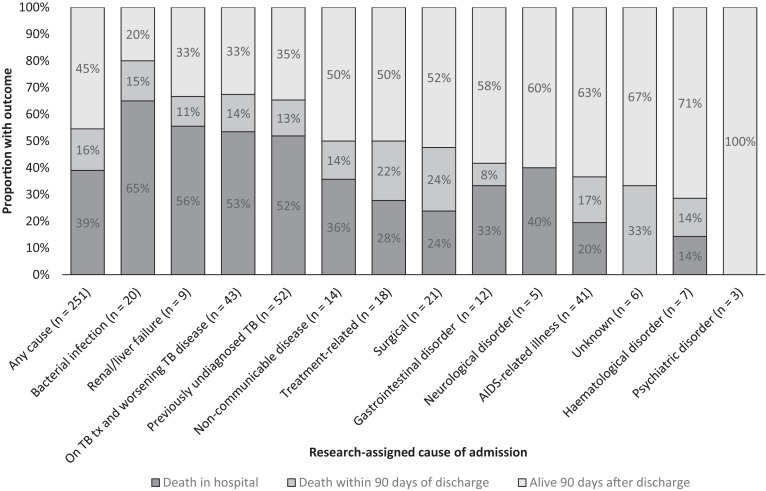
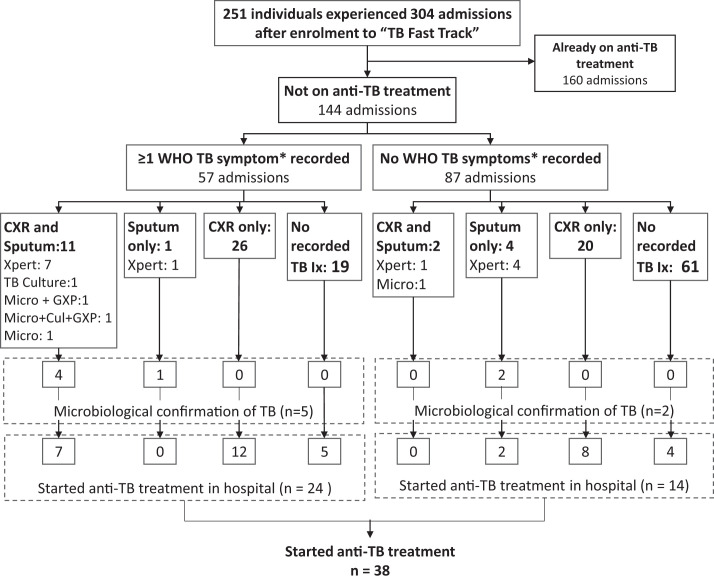
Tuberculosis (TB) remains the leading cause of hospitalization and in-hospital mortality in HIV-positive adults. Using data from hospital and clinic files, research databases, and autopsy, we describe causes and outcomes of admissions, and assess investigations for TB among adults with advanced HIV who were hospitalized after enrollment into the TB Fast Track trial in South Africa (2013-2015). A total of 251 adults [median CD4 count, 37.5 cells/μL; interquartile range, 14-68 cells/µL; 152 (60.6%) on antiretroviral therapy] experienced 304 admissions. Ninety-five of 251 of the first admissions (37.8%) were TB related; the next most common causes were AIDS-related illnesses (41 of 251, 16.3%) and surgical causes (21 of 251, 8.4%). Of those admitted with previously undiagnosed TB, 60% had CD4 counts less than 50 cells/µL. Overall, 137 of 251 individuals died as inpatients or within 90 days of their first discharge. Case fatality rates were particularly high for those admitted with TB (66%) and bacterial infections (80%). In 144 admissions for whom anti-TB treatment had not been started before admission, a sputum-based TB investigation was recorded in only 12 of 57 admissions (21.1%) in whom one or more TB symptom was recorded (24 of 57 started on treatment), and 6 of 87 admissions (6.9%) in whom no TB symptoms were recorded (14 of 87 started on treatment). Hospitalized adults with advanced HIV are at high risk of death. TB was a common cause of hospitalization but was under-investigated, even in those with symptoms. In addition to early identification of TB and other AIDS-related illnesses during hospitalization of adults with advanced HIV, improved pre-hospital management strategies are needed to interrupt disease progression and reduce poor outcomes in this already vulnerable population.
Figures
References
-
- World Health Organization , 2017. Guidelines for Managing Advanced HIV Disease and Rapid Initiation of Antiretroviral Therapy. License: CC BY-NC-SA 3.0 IGO. Geneva, Switzerland: WHO. - PubMed
-
- Egger M. et al., 2002. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet 360: 119–129. - PubMed
-
- Ford N. et al., 2015. Causes of hospital admission among people living with HIV worldwide: a systematic review and meta-analysis. Lancet HIV 2: e438–e444. - PubMed
-
- Perry ME, Kalenga K, Watkins LF, Mukaya JE, Powis KM, Bennett K, Mmalane M, Makhema J, Shapiro RL, 2017. HIV-related mortality at a district hospital in Botswana. Int J STD AIDS 28: 277–283. - PubMed
-
- Akinkuotu A, Roemer E, Richardson A, Namarika DC, Munthali C, Bahling A, Hoffman IF, Hosseinipour MC, 2011. In-hospital mortality rates and HIV: a medical ward review, Lilongwe, Malawi. Int J STD AIDS 22: 465–470. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
