

Clinical added value of MRI to CT in patients scheduled for local therapy of colorectal liver metastases (CAMINO): study protocol for an international multicentre prospective diagnostic accuracy study
- PMID: 34663243
- PMCID: PMC8524830
- DOI: 10.1186/s12885-021-08833-1
Clinical added value of MRI to CT in patients scheduled for local therapy of colorectal liver metastases (CAMINO): study protocol for an international multicentre prospective diagnostic accuracy study
Abstract
Background: Abdominal computed tomography (CT) is the standard imaging method for patients with suspected colorectal liver metastases (CRLM) in the diagnostic workup for surgery or thermal ablation. Diffusion-weighted and gadoxetic-acid-enhanced magnetic resonance imaging (MRI) of the liver is increasingly used to improve the detection rate and characterization of liver lesions. MRI is superior in detection and characterization of CRLM as compared to CT. However, it is unknown how MRI actually impacts patient management. The primary aim of the CAMINO study is to evaluate whether MRI has sufficient clinical added value to be routinely added to CT in the staging of CRLM. The secondary objective is to identify subgroups who benefit the most from additional MRI.
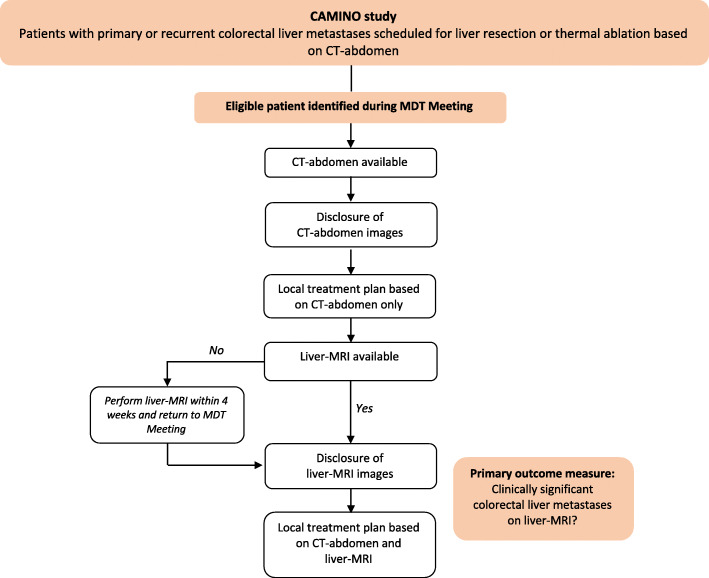
Methods: In this international multicentre prospective incremental diagnostic accuracy study, 298 patients with primary or recurrent CRLM scheduled for curative liver resection or thermal ablation based on CT staging will be enrolled from 17 centres across the Netherlands, Belgium, Norway, and Italy. All study participants will undergo CT and diffusion-weighted and gadoxetic-acid enhanced MRI prior to local therapy. The local multidisciplinary team will provide two local therapy plans: first, based on CT-staging and second, based on both CT and MRI. The primary outcome measure is the proportion of clinically significant CRLM (CS-CRLM) detected by MRI not visible on CT. CS-CRLM are defined as liver lesions leading to a change in local therapeutical management. If MRI detects new CRLM in segments which would have been resected in the original operative plan, these are not considered CS-CRLM. It is hypothesized that MRI will lead to the detection of CS-CRLM in ≥10% of patients which is considered the minimal clinically important difference. Furthermore, a prediction model will be developed using multivariable logistic regression modelling to evaluate the predictive value of patient, tumor and procedural variables on finding CS-CRLM on MRI.
Discussion: The CAMINO study will clarify the clinical added value of MRI to CT in patients with CRLM scheduled for local therapy. This study will provide the evidence required for the implementation of additional MRI in the routine work-up of patients with primary and recurrent CRLM for local therapy.
Trial registration: The CAMINO study was registered in the Netherlands National Trial Register under number NL8039 on September 20th 2019.
Keywords: Abdominal CT scan; Colorectal cancer; Colorectal liver metastases; Diffusion weighted imaging; Gadoxetic acid; Hepatic resection; Liver MRI; Liver metastases; Liver surgery; Thermal ablation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Adam R, de Gramont A, Figueras J, Kokudo N, Kunstlinger F, Loyer E, Poston G, Rougier P, Rubbia-Brandt L, Sobrero A, Teh C, Tejpar S, van Cutsem E, Vauthey JN, Påhlman L, of the EGOSLIM (Expert Group on OncoSurgery management of LIver Metastases) group Managing synchronous liver metastases from colorectal cancer: a multidisciplinary international consensus. Cancer Treat Rev. 2015;41(9):729–741. doi: 10.1016/j.ctrv.2015.06.006. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
