

Eat, breathe, sleep with Osteogenesis Imperfecta
- PMID: 34663416
- PMCID: PMC8522055
- DOI: 10.1186/s13023-021-02058-y
Eat, breathe, sleep with Osteogenesis Imperfecta
Abstract
Background: Although Osteogenesis Imperfecta (OI) affects the connective tissue causing extremely brittle bones with consequent skeletal deformities, it is important to go beyond bones. Indeed, the quality of life in OI does not only depend on bones status, as OI might affect also other important functions. We have therefore implemented a multidisciplinary study to assess lung function, breathing pattern, sleep quality and nutritional status in 27 adult OI type III and IV patients (median age: 34.6 years; 19 women; 14 type III).
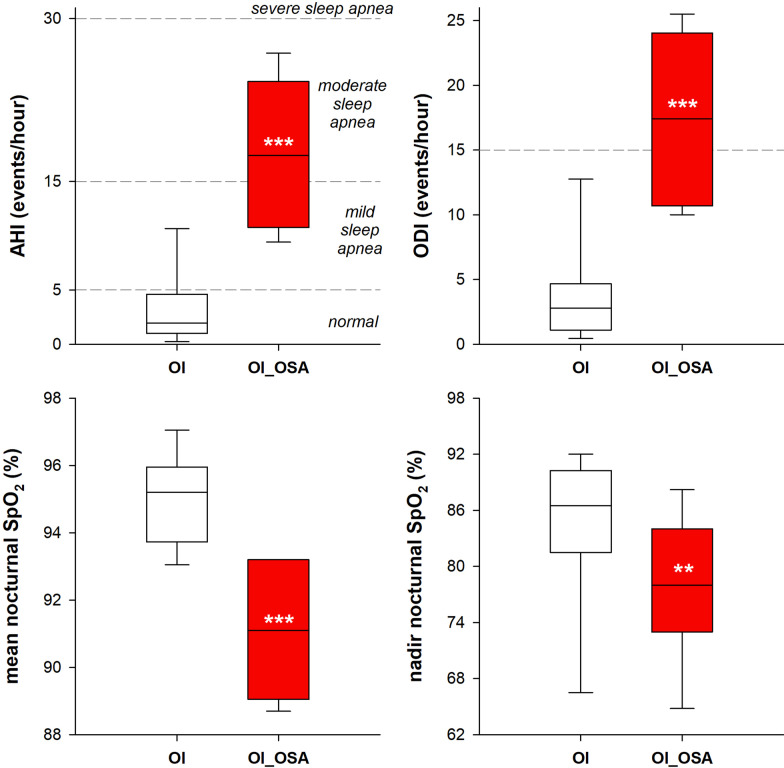
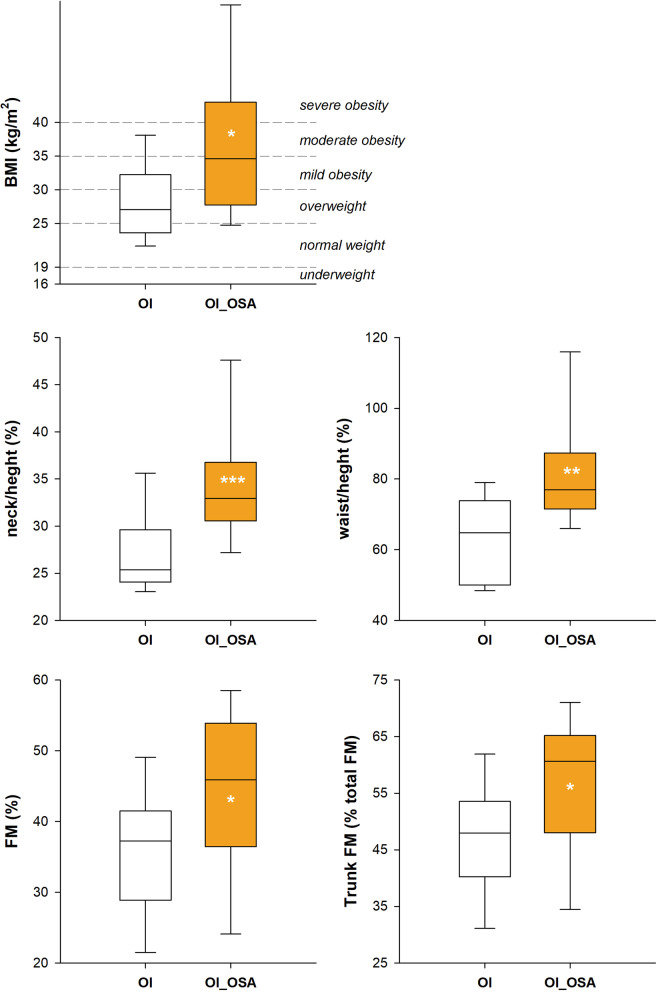
Results: According to nocturnal oxygen desaturation, two groups were identified: 13 patients with (OI_OSA, incidence: 48.2%) and 14 without (no_OSA) obstructive sleep apnea. The former was characterized by higher spinal and ribcage deformity, by more restrictive lung function, by paradoxical thoracic breathing in supine position, by rapid and shallow breathing, by higher body mass index, by longer neck and waist circumferences; by higher abdominal volume and by greater percentage of body fat mass, particularly localized in the trunk. The best predictor of OI_OSA was the negative value of the supine ribcage contribution to tidal volume, followed by the ratio between the neck and the waist circumferences with body height and the supine thoraco-abdominal volumes phase shift angle.
Conclusions: The pathophysiology of OI ensued a dangerous vicious circle, in which breathing, sleep and nutritional status are tightly linked, and they might all end up in negatively affecting the quality of life. The vicious circle is fed by some intrinsic characteristics of the disease (thoracic, cranial and mandibular deformities) and some bad daily habits of the patients (i.e. physical inactivity and low dietary quality). The former impacts on restricting the respiratory function, the latter makes Olers more prone to experience overweight or obesity. The main consequence is a high incidence of obstructive sleep apnea, which remains an underdiagnosed disorder in individuals with severe OI who are obese, with a neck to height ratio over than 31.6%, and characterized by paradoxical breathing in supine position. A multidisciplinary approach, including evaluations of breathing, sleep and nutrition, is required to better manage the disease and fulfil the maximizing well-being of OI patients.
Keywords: AHI index; Body composition; Fat mass; Mediterranean diet; Non-invasive ventilation; Obstructive sleep apnea; Opto-electronic plethysmography; Osteogenesis Imperfecta; Scoliosis; Spirometry.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures






References
-
- Subramanian S, Viswanathan VK. Osteogenesis Imperfecta. StatPearls. 2021 [cited 2021 Jun 1]. - PubMed
-
- Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet. 2004;363:1377–1385. - PubMed
-
- Van Dijk FS, Pals G, Van Rijn RR, Nikkels PGJ, Cobben JM. Classification of Osteogenesis imperfecta revisited. Eur J Med Genet. 2010;53:1–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
