

Avelumab for platinum-ineligible/refractory recurrent and/or metastatic squamous cell carcinoma of the head and neck: phase Ib results from the JAVELIN Solid Tumor trial
- PMID: 34663640
- PMCID: PMC8524383
- DOI: 10.1136/jitc-2021-002998
Avelumab for platinum-ineligible/refractory recurrent and/or metastatic squamous cell carcinoma of the head and neck: phase Ib results from the JAVELIN Solid Tumor trial
Abstract
Background: Recurrent and/or metastatic (R/M) disease develops in approximately 65% of patients with squamous cell carcinoma of the head and neck (SCCHN) and is associated with a poor prognosis. Immune checkpoint inhibitors have proven effective in multiple tumor types, including R/M SCCHN. We report the efficacy and safety of avelumab (antiprogrammed death ligand 1 antibody) in an expansion cohort of patients with platinum-refractory/ineligible R/M SCCHN enrolled in the phase I JAVELIN Solid Tumor trial (NCT01772004).
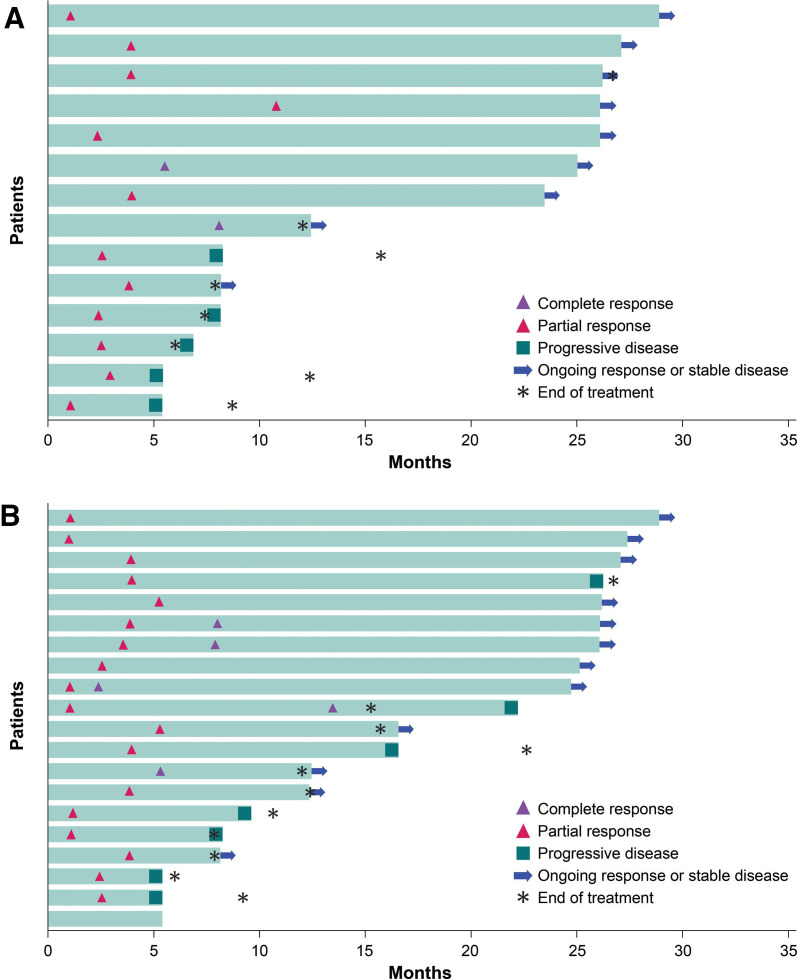
Methods: Eligible patients with R/M SCCHN were aged ≥18 years and had received ≥1 line of platinum-based chemotherapy with disease progression or recurrence within 6 months of the last dose or were ineligible for platinum-based chemotherapy. All patients received avelumab 10 mg/kg every 2 weeks. Tumor assessments were carried out by a blinded independent review committee (IRC) and investigators according to Response Evaluation Criteria in Solid Tumors V.1.1 (RECIST 1.1). Key endpoints included best overall response, duration of response (DOR) and progression-free survival (PFS) assessed by IRC and investigator per RECIST 1.1, overall survival (OS), and safety.
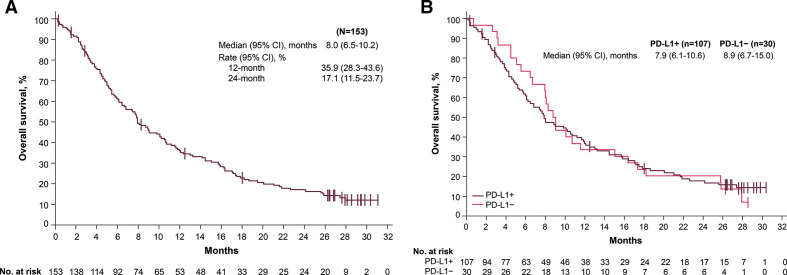
Results: Between April 24, 2015, and November 13, 2015, 153 patients were enrolled. Patients had a median of two prior lines of therapy for metastatic or locally advanced disease (range 0-6); 12 patients (7.8%) were not eligible for platinum-based chemotherapy. At data cut-off (December 31, 2017), the confirmed objective response rate was 9.2% (95% CI 5.1% to 14.9%) assessed by IRC and 13.1% (95% CI 8.2% to 19.5%) assessed by investigator. Median DOR was not reached (95% CI 4.2 to not estimable) based on IRC assessment. Median PFS was 1.4 months (95% CI 1.4 to 2.6) assessed by IRC and 1.8 months (95% CI 1.4 to 2.7) assessed by investigator; median OS was 8.0 months (95% CI 6.5 to 10.2). Any-grade treatment-related adverse events (TRAEs) occurred in 83 patients (54.2%) and were grade ≥3 in 10 patients (6.5%). The most common TRAEs were fatigue (n=19, 12.4%), fever (n=14, 9.2%), pruritus (n=12, 7.8%), and chills (n=11, 7.2%), and there were no treatment-related deaths.
Conclusion: Avelumab showed clinical activity and was associated with a low rate of grade ≥3 TRAEs in heavily pretreated patients with platinum-refractory/ineligible R/M SCCHN.
Keywords: head and neck neoplasms; immunotherapy.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JG reports providing a consulting or advisory role for AstraZeneca, Bristol Myers Squibb, Merck, MSD, Nanobiotix, and Innate Pharma; and has received research funding from Bristol Myers Squibb, Chugai Pharmaceutical Co., Merck and GlaxoSmithKline. K-WL reports providing a consulting or advisory role for Bayer and ISU ABXIS; has received honoraria from Bristol Myers Squibb, Eli Lilly, and Genexine; and received research funding from ABL Bio, ALX Oncology, AstraZeneca/MedImmune, BeiGene, Daiichi Sankyo, Five Prime Therapeutics, GC Pharma, Genexine, LSK BioPharma, MacroGenics, MSD, Merck, Oncologie, Ono Pharmaceutical, Pfizer, Pharmacyclics, Taiho Pharmaceutical, Y-BIOLOGICS, and Zymeworks (to his institution for conducting clinical trials). MRP has received honoraria from AbbVie, Bayer, Genentech, Janssen Pharmaceutical, Pharmacyclics, and Pfizer; provided speakers services for Celgene, Merck, and Exelixis; and research funding from Acerta Pharma, ADC Therapeutics, Agenus, Aileron Therapeutics, AstraZeneca, Bicycle Therapeutics, BioNTech, Boehringer Ingelheim, Calithera Biosciences, Celgene, Checkpoint Therapeutics, Ciclomed, Covis Pharma, Curis, Cyteir Therapeutics, Daiichi Sankyo, eFFECTOR Therapeutics, Eli Lilly, Merck, Evelo Biosciences, Forma Therapeutics, Genentech/Roche, Gilead, GlaxoSmithKline, H3 Biomedicine, Hengrui Therapeutics, Hutchinson MediPharma, Ignyta, Incyte, Jacobio Pharmaceuticals, Janssen Pharmaceutical, Jounce Therapeutics, KLUS Pharma, Kymab, Loxo Oncology, LSK Biopartners, Lycera, MacroGenics, Merck, Millennium Pharmaceuticals, Mirati Therapeutics, Moderna, Pfizer, Phoenix Molecular Designs, Placon Therapeutics, Portola Pharmaceuticals, Prelude Therapeutics, Qilu Puget Sound Biotherapeutics, Revolution Medicines, Ribon Therapeutics, Seven and Eight Biopharmaceuticals, Stemline Therapeutics, Syndax, Synthorx, Taiho Pharmaceutical, Takeda, Tesaro, TopAlliance, Vedanta Biosciences, Verastem Oncology, Vigeo Therapeutics, and Xencor. AD reports providing a consulting or advisory role for and receiving reimbursement for travel and accommodation expenses from Bristol Myers Squibb and Merck. DW reports providing a consulting or advisory role for Bristol Myers Squibb and Sanofi-Aventis, and has received research funding from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Enzychem Lifesciences, F-star, Genentech, Iovance Biotherapeutics, Kura Oncology, MSD, Merck, Pfizer, Regeneron, and Sanofi. MSG reports providing a consulting or advisory role for Deciphera Pharmaceuticals, ImaginAb, Redhill Biopharma, and TRACON Pharmaceuticals; and owns stock in Caremission and Medilus. MG reports providing a consulting or advisory role for Guardant360; speakers services for Merck; has received research funding from Array Biopharma, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Care Progress, Celgene, Compass Therapeutics, Constellation Pharmaceuticals, CytRx, Eisai, Esanex, Genentech, Incyte, Infinity Pharmaceuticals, Janssen, Karyopharm Therapeutics, MedImmune, Merck, Mirati Therapeutics, Moderna, Pfizer, Regeneron, Sanofi, Seattle Genetics, Tesaro, and Vendata Biosciences; owns stock in Cota Healthcare; and is an employee of Reginal Cancer Care Associates. AB reports providing speakers services for AstraZeneca, Bristol Myers Squibb, Eli Lilly, Genentech, and Merck; and has received research funding from Arcus Biosciences, Bristol Myers Squibb, Genentech, GlaxoSmithKline, MedImmune, and Merck. CLT has received honoraria from Amgen, AstraZeneca, Bristol Myers Squibb, Merck, GlaxoSmithKline, MSD, Nanobiotix, Rakuten, Roche, and Seattle Genetics; provided a consulting or advisory role for Idem Healthcare; and reimbursement for travel and accommodation expenses from AstraZeneca, Bristol Myers Squibb, Merck, and MSD. DV reports providing a consulting or advisory role for Nestlé and Nutricia. PS has received honoraria from Blueprint Medicines, Boehringer Ingelheim, and Deciphera Pharmaceuticals; provided a consulting or advisory role for Adaptimmune, Advanced Medical, Blueprint Medicines, Boehringer Ingelheim, Deciphera, Ellipses Pharma, Exelixis, Guided Clarity, Intellisphere, Medscape, and Transgene; research funding from CoBioRes, Eisai, G1 Therapeutics, Novartis, and PharmaMar; and reimbursement for travel and accommodation expenses from Boehringer Ingelheim, Ipsen, and MSD. HJG is an employee of Merck Healthcare KGaA, Darmstadt, Germany. DZ is an employee of Merck Serono (Beijing) Pharmaceutical R&D Co., Ltd. Beijing, China, an affiliate of Merck KGaA. MB is an employee of Merck Healthcare KGaA, Darmstadt, Germany. All other authors have nothing to disclose.
Figures

References
-
- Blot WJ, McLaughlin JK, Winn DM, et al. . Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 1988;48:3282–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous