

Assessing and predicting adolescent and early adulthood common mental disorders using electronic primary care data: analysis of a prospective cohort study (ALSPAC) in Southwest England
- PMID: 34663669
- PMCID: PMC8524296
- DOI: 10.1136/bmjopen-2021-053624
Assessing and predicting adolescent and early adulthood common mental disorders using electronic primary care data: analysis of a prospective cohort study (ALSPAC) in Southwest England
Abstract
Objectives: We aimed to examine agreement between common mental disorders (CMDs) from primary care records and repeated CMD questionnaire data from ALSPAC (the Avon Longitudinal Study of Parents and Children) over adolescence and young adulthood, explore factors affecting CMD identification in primary care records, and construct models predicting ALSPAC-derived CMDs using only primary care data.
Design and setting: Prospective cohort study (ALSPAC) in Southwest England with linkage to electronic primary care records.
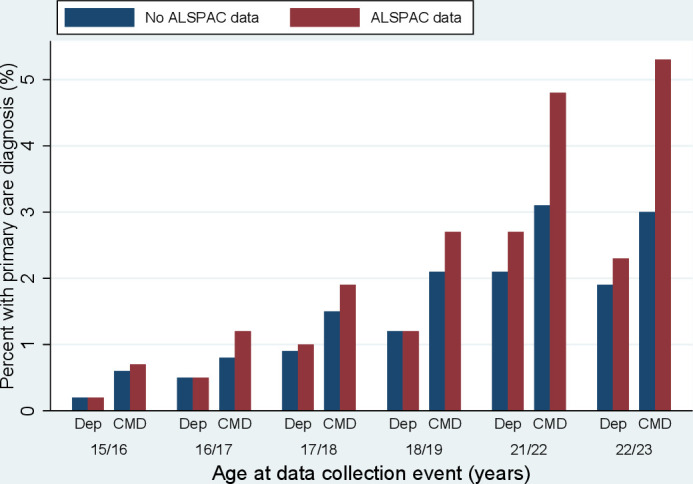
Participants: Primary care records were extracted for 11 807 participants (80% of 14 731 eligible). Between 31% (3633; age 15/16) and 11% (1298; age 21/22) of participants had both primary care and ALSPAC CMD data.
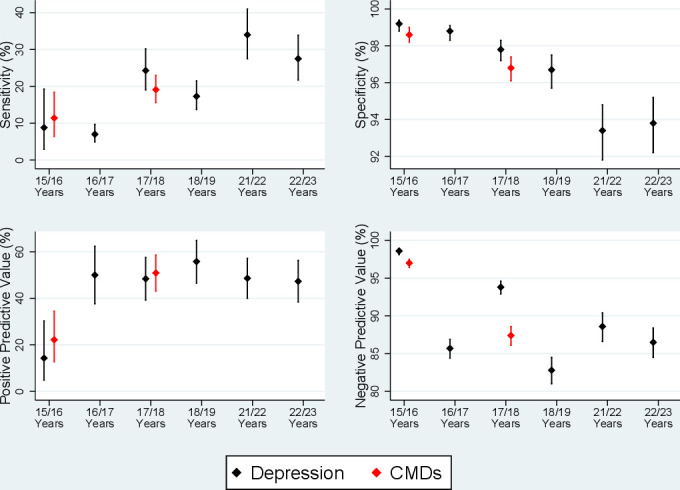
Outcome measures: ALSPAC outcome measures were diagnoses of suspected depression and/or CMDs. Primary care outcome measure were Read codes for diagnosis, symptoms and treatment of depression/CMDs. For each time point, sensitivities and specificities for primary care CMD diagnoses were calculated for predicting ALSPAC-derived measures of CMDs, and the factors associated with identification of primary care-based CMDs in those with suspected ALSPAC-derived CMDs explored. Lasso (least absolute selection and shrinkage operator) models were used at each time point to predict ALSPAC-derived CMDs using only primary care data, with internal validation by randomly splitting data into 60% training and 40% validation samples.
Results: Sensitivities for primary care diagnoses were low for CMDs (range: 3.5%-19.1%) and depression (range: 1.6%-34.0%), while specificities were high (nearly all >95%). The strongest predictors of identification in the primary care data for those with ALSPAC-derived CMDs were symptom severity indices. The lasso models had relatively low prediction rates, especially in the validation sample (deviance ratio range: -1.3 to 12.6%), but improved with age.
Conclusions: Primary care data underestimate CMDs compared to population-based studies. Improving general practitioner identification, and using free-text or secondary care data, is needed to improve the accuracy of models using clinical data.
Keywords: anxiety disorders; child & adolescent psychiatry; depression & mood disorders; epidemiology; primary care.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Disagreement concerning atopic dermatitis subtypes between an English prospective cohort (ALSPAC) and linked electronic health records.Clin Exp Dermatol. 2024 Nov 22;49(12):1537-1546. doi: 10.1093/ced/llae196. Clin Exp Dermatol. 2024. PMID: 38751343 Free PMC article.
-
Defining adolescent common mental disorders using electronic primary care data: a comparison with outcomes measured using the CIS-R.BMJ Open. 2016 Dec 1;6(12):e013167. doi: 10.1136/bmjopen-2016-013167. BMJ Open. 2016. PMID: 27909036 Free PMC article.
-
Tracking the course of depressive and anxiety symptoms across adolescence (the CATS study): a population-based cohort study in Australia.Lancet Psychiatry. 2025 Jan;12(1):44-53. doi: 10.1016/S2215-0366(24)00361-4. Epub 2024 Dec 4. Lancet Psychiatry. 2025. PMID: 39644904
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Digital Interventions for Screening and Treating Common Mental Disorders or Symptoms of Common Mental Illness in Adults: Systematic Review and Meta-analysis.J Med Internet Res. 2020 Sep 2;22(9):e20581. doi: 10.2196/20581. J Med Internet Res. 2020. PMID: 32876577 Free PMC article.
Cited by
-
Disagreement concerning atopic dermatitis subtypes between an English prospective cohort (ALSPAC) and linked electronic health records.Clin Exp Dermatol. 2024 Nov 22;49(12):1537-1546. doi: 10.1093/ced/llae196. Clin Exp Dermatol. 2024. PMID: 38751343 Free PMC article.
-
Preconception indicators and associations with health outcomes reported in UK routine primary care data: a systematic review.Br J Gen Pract. 2025 Jan 30;75(751):e129-e136. doi: 10.3399/BJGP.2024.0082. Print 2025 Feb. Br J Gen Pract. 2025. PMID: 38950944 Free PMC article.
-
Psychotic experiences and disorders in adolescents and young adults with borderline intellectual functioning and intellectual disabilities: evidence from a population-based birth cohort in the United Kingdom.Psychol Med. 2025 Feb 5;55:e23. doi: 10.1017/S0033291724003556. Psychol Med. 2025. PMID: 39905820 Free PMC article.
-
The relationship between cognitive and affective control and adolescent mental health.JCPP Adv. 2023 Nov 3;4(1):e12204. doi: 10.1002/jcv2.12204. eCollection 2024 Mar. JCPP Adv. 2023. PMID: 38486950 Free PMC article.
-
Mental Health Difficulties in Children who Develop Misophonia: An Examination of ADHD, Depression & Anxiety.Child Psychiatry Hum Dev. 2025 Apr;56(2):520-532. doi: 10.1007/s10578-023-01569-y. Epub 2023 Jul 28. Child Psychiatry Hum Dev. 2025. PMID: 37501042 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical