

Predicting cancer outcomes with radiomics and artificial intelligence in radiology
- PMID: 34663898
- PMCID: PMC9034765
- DOI: 10.1038/s41571-021-00560-7
Predicting cancer outcomes with radiomics and artificial intelligence in radiology
Abstract
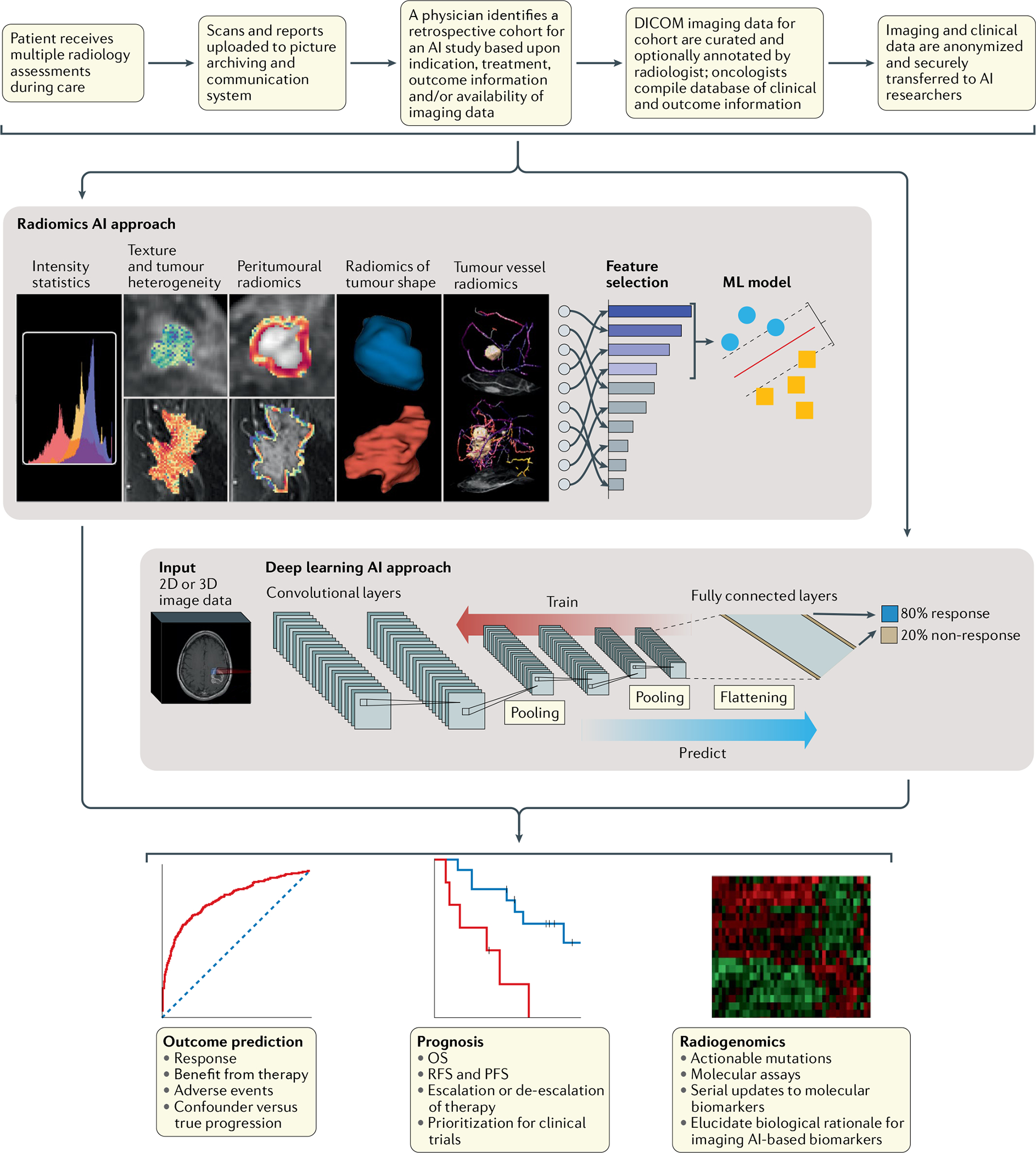
The successful use of artificial intelligence (AI) for diagnostic purposes has prompted the application of AI-based cancer imaging analysis to address other, more complex, clinical needs. In this Perspective, we discuss the next generation of challenges in clinical decision-making that AI tools can solve using radiology images, such as prognostication of outcome across multiple cancers, prediction of response to various treatment modalities, discrimination of benign treatment confounders from true progression, identification of unusual response patterns and prediction of the mutational and molecular profile of tumours. We describe the evolution of and opportunities for AI in oncology imaging, focusing on hand-crafted radiomic approaches and deep learning-derived representations, with examples of their application for decision support. We also address the challenges faced on the path to clinical adoption, including data curation and annotation, interpretability, and regulatory and reimbursement issues. We hope to demystify AI in radiology for clinicians by helping them to understand its limitations and challenges, as well as the opportunities it provides as a decision-support tool in cancer management.
© 2021. Springer Nature Limited.
Conflict of interest statement
Competing interests
N.B. is a current employee of Tempus Labs and a former employee of IBM Research, with both of which he is an inventor on several pending patents pertaining to medical image analysis. He additionally holds equity in Tempus Labs. V.V. is a consultant for Alkermes, AstraZeneca, Bristol Myers Squibb, Celgene, Foundation Medicine, Genentech, Merck, Nektar Therapeutics and Takeda, has current or pending grants from Alkermes, AstraZeneca, Bristol Myers Squibb, Genentech and Merck, is on the speakers’ bureaus of Bristol Myers Squibb, Celgene, Foundation Medicine and Novartis, and has received payment for the development of educational presentations from Bristol Myers Squibb and Foundation Medicine. A.M. holds equity in Elucid Bioimaging and Inspirata, has been or is a scientific advisory board member for Aiforia, AstraZeneca, Bristol Myers Squibb, Inspirata and Merck, serves as a consultant for Caris, Inc. and Roche Diagnostics, has sponsored research agreements with AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb and Philips, has developed a technology relating to cardiovascular imaging that has been licensed to Elucid Bioimaging, and is involved in an NIH U24 grant with PathCore and three different NIH R01 grants with Inspirata. The other authors declare no competing interests.
Figures
References
-
- Giger ML, Doi K & MacMahon H Computerized detection of lung nodules in digital chest radiographs. Med. Imaging Proc. 767, 384–387 (1987).
-
- Carmody DP, Nodine CF & Kundel HL An analysis of perceptual and cognitive factors in radiographic interpretation. Perception 9, 339–344 (1980). - PubMed
-
- Kundel HL & Hendee WR The perception of radiologic image information. Report of an NCI workshop on April 15–16, 1985. Invest. Radiol. 20, 874–877 (1985). - PubMed
-
- Rao VM et al. How widely Is computer-aided detection used in screening and diagnostic mammography? J. Am. Coll. Radiol. 7, 802–805 (2010). - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR002548/TR/NCATS NIH HHS/United States
- R01 CA216579/CA/NCI NIH HHS/United States
- T32 EB007509/EB/NIBIB NIH HHS/United States
- IK6 BX006185/BX/BLRD VA/United States
- U24 CA199374/CA/NCI NIH HHS/United States
- R43 EB028736/EB/NIBIB NIH HHS/United States
- U01 CA239055/CA/NCI NIH HHS/United States
- R01 HL158071/HL/NHLBI NIH HHS/United States
- F31 CA221383/CA/NCI NIH HHS/United States
- R01 CA249992/CA/NCI NIH HHS/United States
- R01 HL151277/HL/NHLBI NIH HHS/United States
- R01 CA220581/CA/NCI NIH HHS/United States
- R01 CA202752/CA/NCI NIH HHS/United States
- R01 CA208236/CA/NCI NIH HHS/United States
- R43 EB015199/EB/NIBIB NIH HHS/United States
- C06 RR012463/RR/NCRR NIH HHS/United States
- U01 CA248226/CA/NCI NIH HHS/United States
- I01 BX004121/BX/BLRD VA/United States
- R01 CA257612/CA/NCI NIH HHS/United States
- U54 CA254566/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
