

Lung neuroendocrine neoplasms: recent progress and persistent challenges
- PMID: 34663914
- PMCID: PMC8695375
- DOI: 10.1038/s41379-021-00943-2
Lung neuroendocrine neoplasms: recent progress and persistent challenges
Abstract
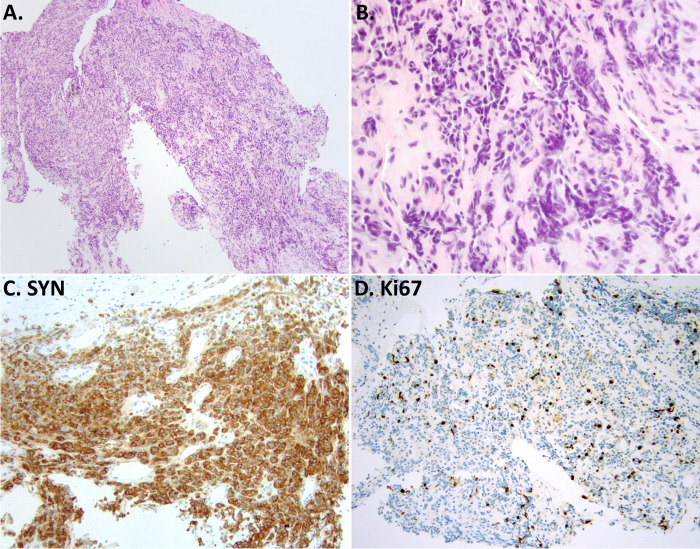
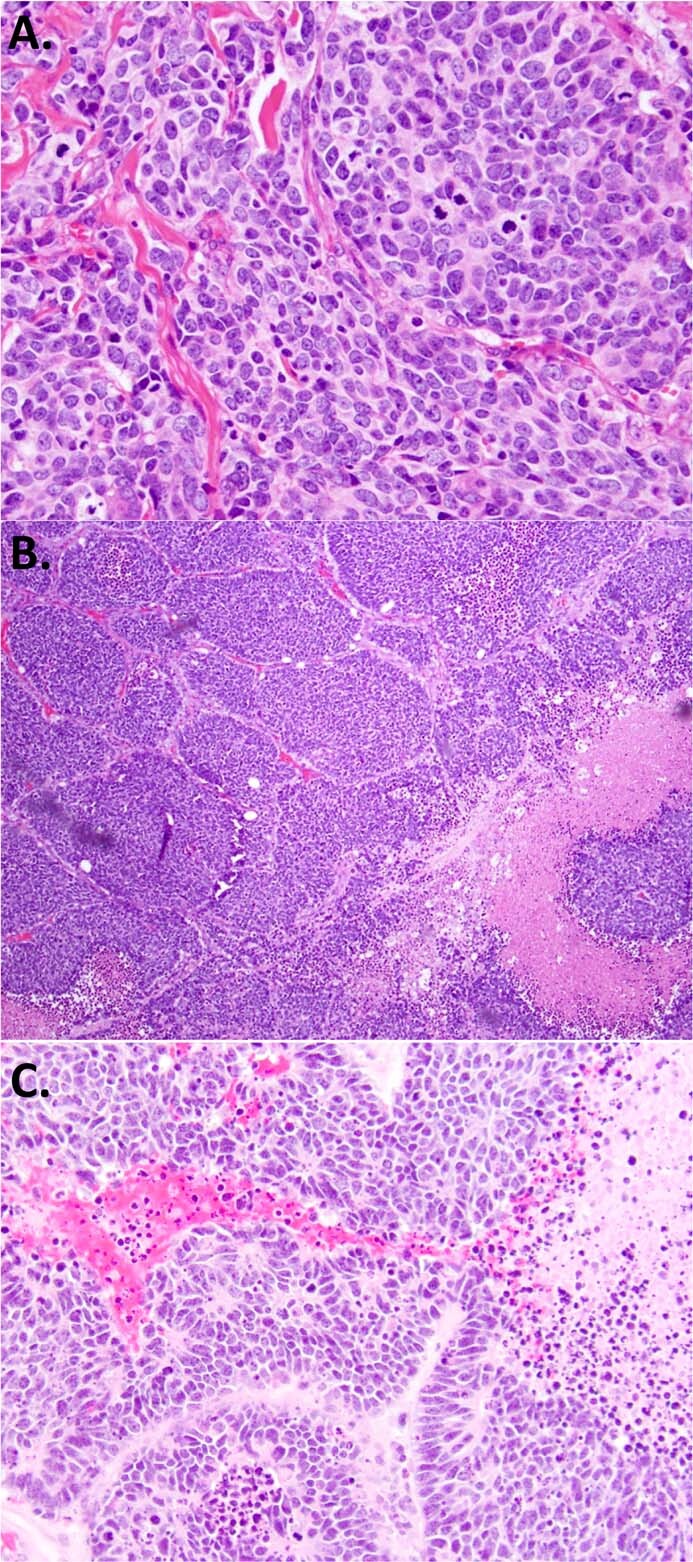
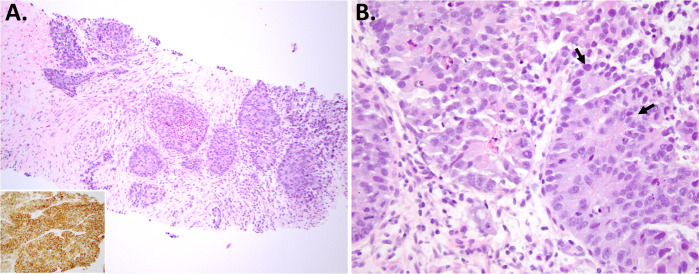
This review summarizes key recent developments relevant to the pathologic diagnosis of lung neuroendocrine neoplasms, including carcinoids, small cell lung carcinoma (SCLC), and large cell neuroendocrine carcinoma (LCNEC). Covered are recent insights into the biological subtypes within each main tumor type, progress in pathological diagnosis and immunohistochemical markers, and persistent challenging areas. Highlighted topics include highly proliferative carcinoids and their distinction from small cell and large cell neuroendocrine carcinomas (NECs), the evolving role of Ki67, the update on the differential diagnosis of NEC to include thoracic SMARCA4-deficient undifferentiated tumors, the recent data on SCLC transcriptional subtypes with the emergence of POU2F3 as a novel marker for the diagnosis of SCLC with low/negative expression of standard neuroendocrine markers, and the update on the diagnosis of LCNEC, particularly in biopsies. There has been remarkable recent progress in the understanding of the genetic and expression-based profiles within each type of lung neuroendocrine neoplasm, and it is hoped that these insights will enable the development of novel diagnostic, prognostic, and predictive biomarkers to aid in the pathologic assessment of these tumors in the future.
© 2021. The Author(s).
Conflict of interest statement
The author declares no competing interests.
Figures




References
-
- WHO Classification of Tumours Editorial Board. Thoracic Tumours. 5th ed. Lyon (France): International Agency for Research on Cancer. (2021).
-
- Rekhtman N. Neuroendocrine tumors of the lung: an update. Arch. Pathol. Lab. Med. 2010;134:1628–1638. - PubMed
-
- WHO Classification of Tumours Editorial Board. Digestive System Tumours. 5th ed. Lyon (France): International Agency for Research on Cancer. (2019).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
