

The microbiome of dental and peri-implant subgingival plaque during peri-implant mucositis therapy: A randomized clinical trial
- PMID: 34664294
- PMCID: PMC9298297
- DOI: 10.1111/jcpe.13566
The microbiome of dental and peri-implant subgingival plaque during peri-implant mucositis therapy: A randomized clinical trial
Abstract
Aim: To assess the microbial effects of mechanical debridement in conjunction with a mouthrinse on sites with peri-implant mucositis and gingivitis.
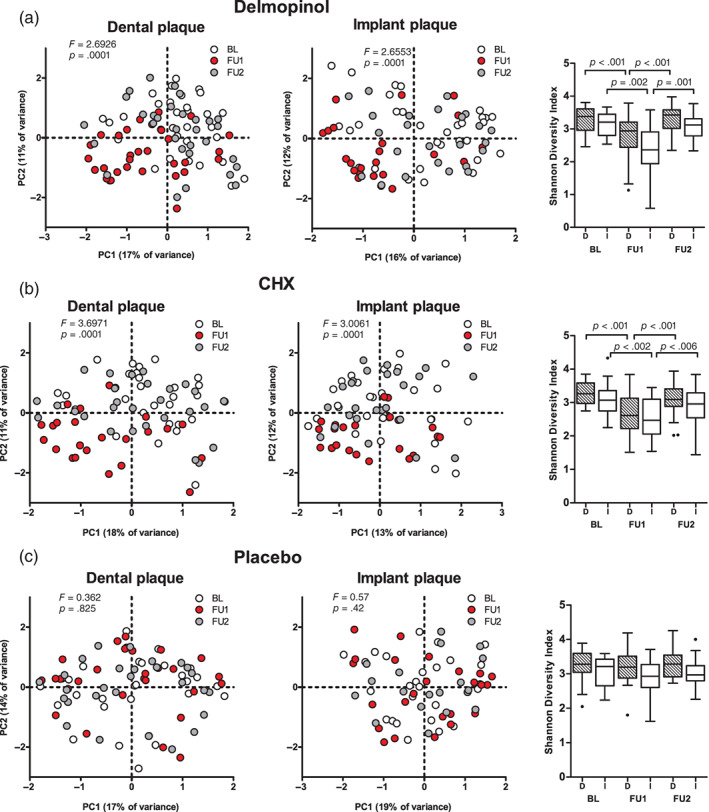
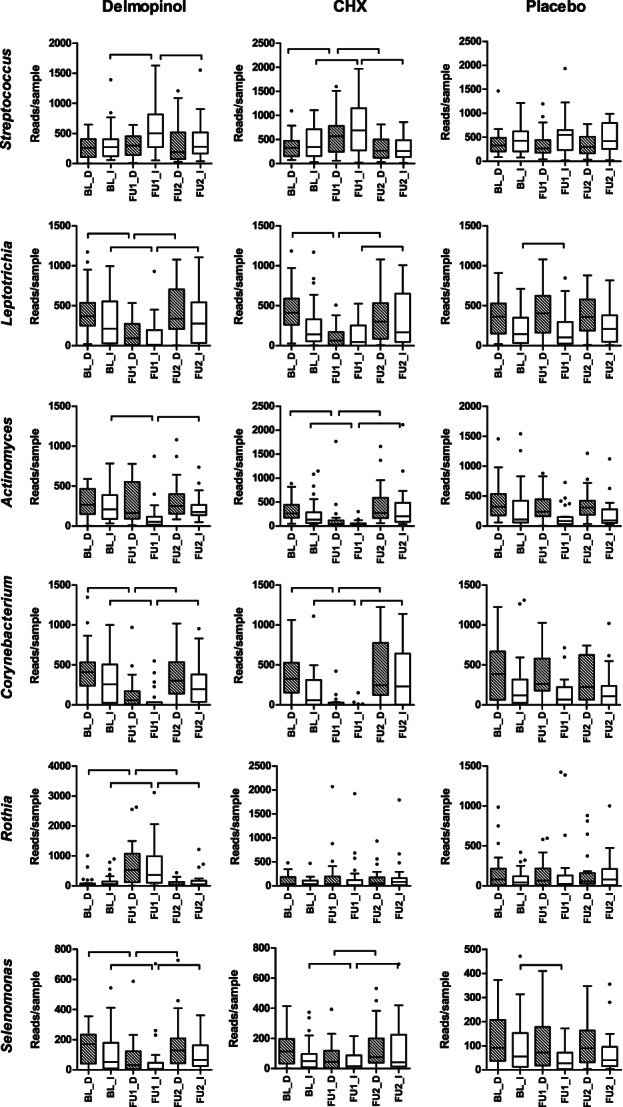
Materials and methods: Eighty-nine patients with peri-implant mucositis were included in a double-blinded, randomized, placebo-controlled trial with mechanical debridement and 1-month use of either delmopinol, chlorhexidine (CHX), or a placebo mouthrinse. Submucosal and subgingival plaque samples of implants and teeth were collected at baseline and after 1 and 3 months, processed for 16S V4 rRNA gene amplicon sequencing, and analysed bioinformatically.
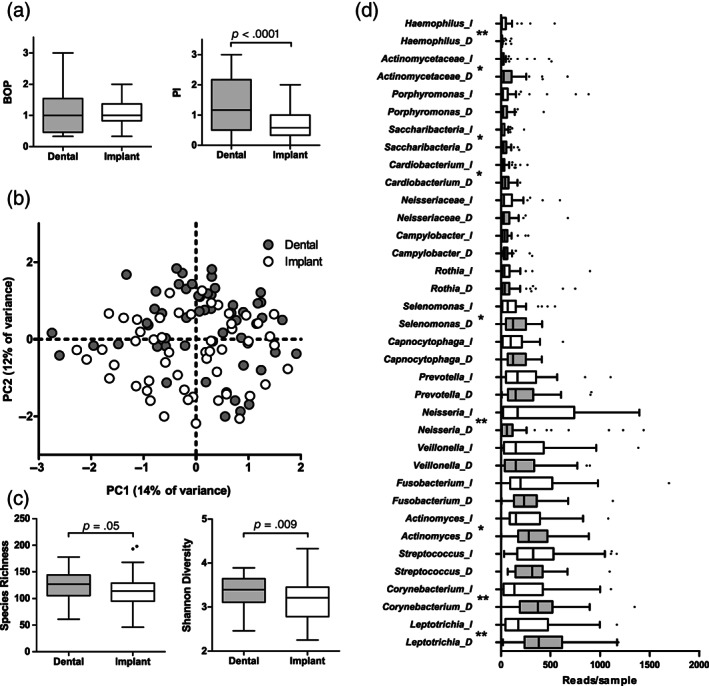
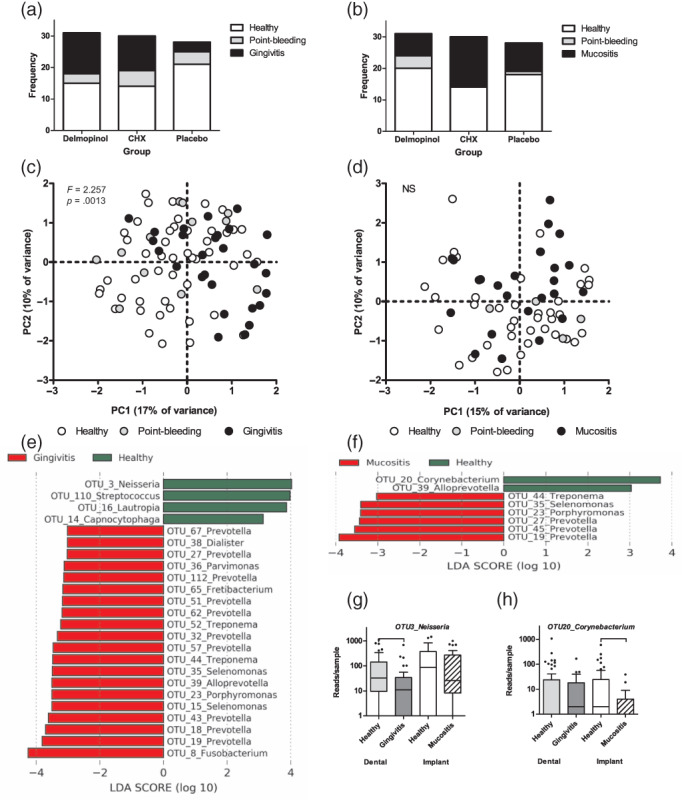
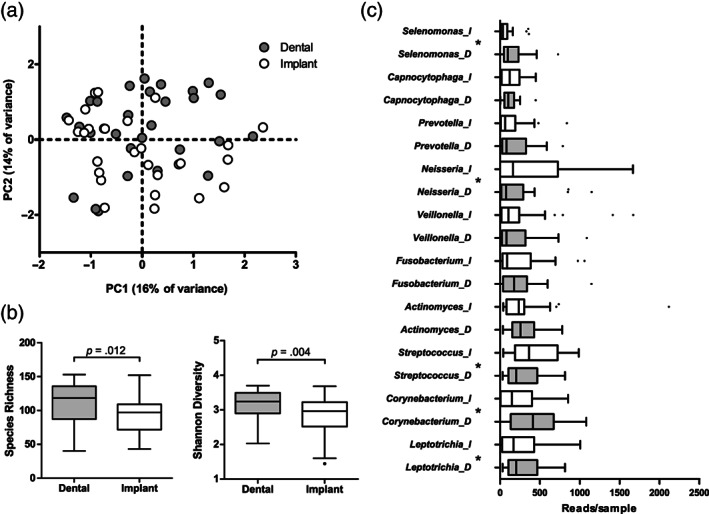
Results: The sites with peri-implant mucositis presented with a less diverse and less anaerobic microbiome. Exposure to delmopinol or CHX, but not to the placebo mouthrinse resulted in microbial changes after 1 month. The healthy sites around the teeth harboured a more diverse and more anaerobe-rich microbiome than the healthy sites around the implants.
Conclusions: Peri-implant sites with mucositis harbour ecologically less complex and less anaerobic biofilms with lower biomass than patient-matched dental sites with gingivitis while eliciting an equal inflammatory response. Adjunctive antimicrobial therapy in addition to mechanical debridement does affect both dental and peri-implant biofilm composition in the short term, resulting in a less dysbiotic subgingival biofilm.
Keywords: chlorhexidine; delmopinol; dental implant; microbiome; peri-implant mucositis; subgingival plaque; submucosal plaque.
© 2021 The Authors. Journal of Clinical Periodontology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
-
- Belibasakis, G. N. (2014). Microbiological and immuno‐pathological aspects of peri‐implant diseases. Archives of Oral Biology, 59, 66–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
