

18F-MK-6240 tau-PET in genetic frontotemporal dementia
- PMID: 34664612
- PMCID: PMC9166561
- DOI: 10.1093/brain/awab392
18F-MK-6240 tau-PET in genetic frontotemporal dementia
Abstract
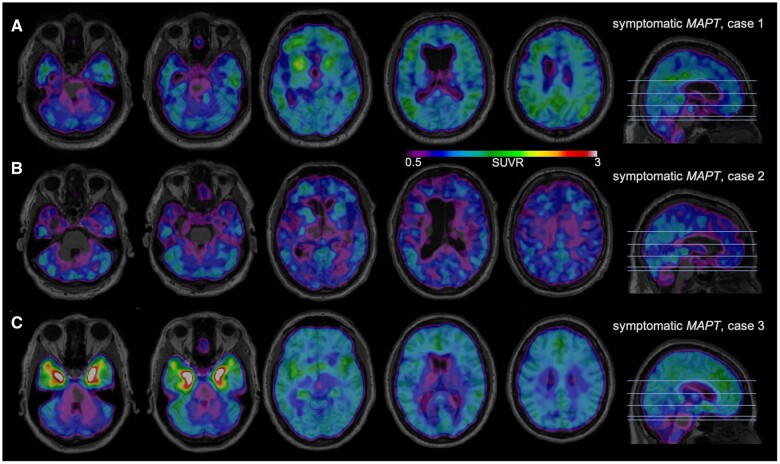
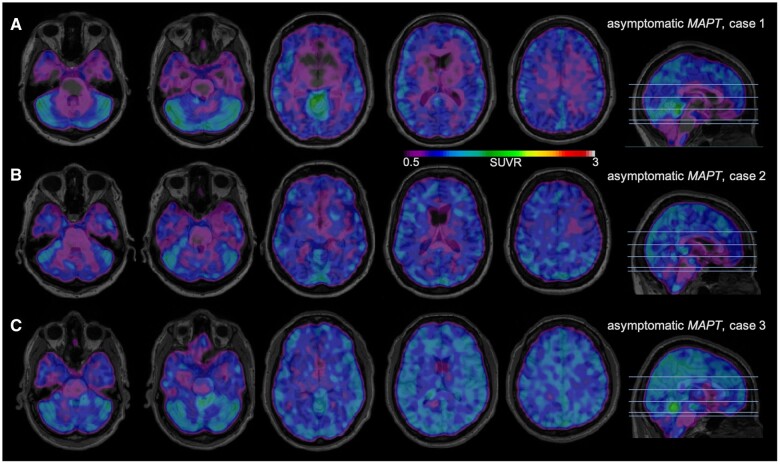
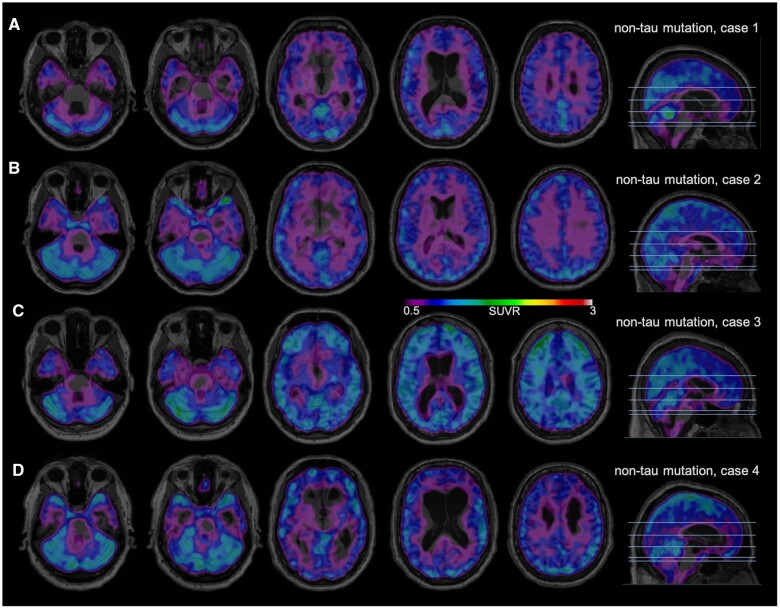
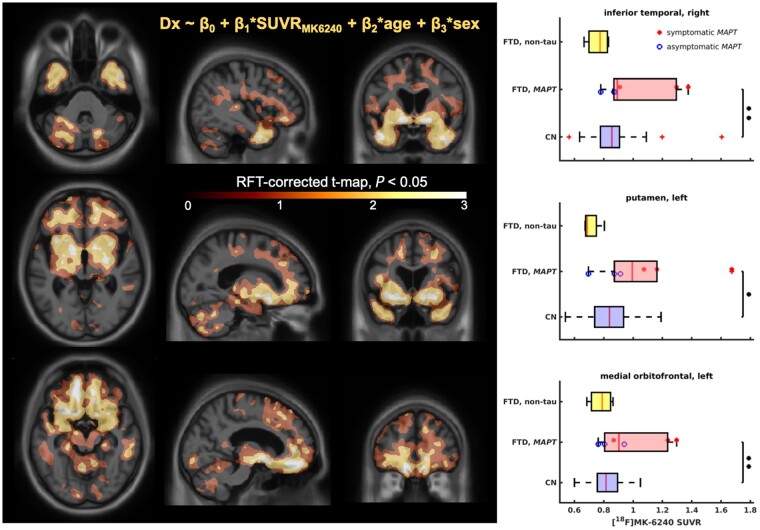
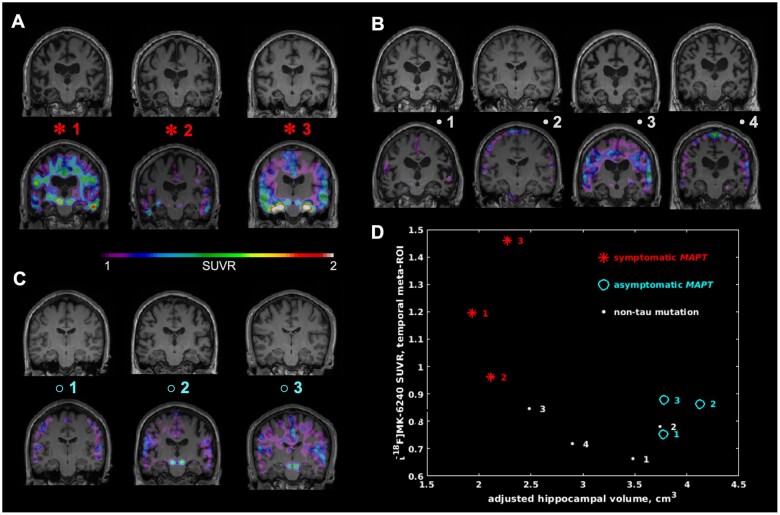
Tau is one of several proteins associated with frontotemporal dementia. While knowing which protein is causing a patient's disease is crucial, no biomarker currently exists for identifying tau in vivo in frontotemporal dementia. The objective of this study was to investigate the potential for the promising 18F-MK-6240 PET tracer to bind to tau in vivo in genetic frontotemporal dementia. We enrolled subjects with genetic frontotemporal dementia, who constitute an ideal population for testing because their pathology is already known based on their mutation. Ten participants (three with symptomatic P301L and R406W MAPT mutations expected to show tau binding, three with presymptomatic MAPT mutations and four with non-tau mutations who acted as disease controls) underwent clinical characterization, tau-PET scanning with 18F-MK-6240, amyloid-PET imaging with 18F-NAV-4694 to rule out confounding Alzheimer's pathology, and high-resolution structural MRI. Tau-PET scans of all three symptomatic MAPT carriers demonstrated at least mild 18F-MK-6240 binding in expected regions, with particularly strong binding in a subject with an R406W MAPT mutation (known to be associated with Alzheimer's like neurofibrillary tangles). Two asymptomatic MAPT carriers estimated to be 5 years from disease onset both showed modest 18F-MK-6240 binding, while one ∼30 years from disease onset did not exhibit any binding. Additionally, four individuals with symptomatic frontotemporal dementia caused by a non-tau mutation were scanned (two C9orf72; one GRN; one VCP): 18F-MK-6240 scans were negative for three subjects, while one advanced C9orf72 case showed minimal regionally non-specific binding. All 10 amyloid-PET scans were negative. Furthermore, a general linear model contrasting genetic frontotemporal dementia subjects to a set of 83 age-matched controls showed significant binding only in the MAPT carriers in selected frontal, temporal and subcortical regions. In summary, our findings demonstrate mild but significant binding of MK-6240 in amyloid-negative P301L and R406W MAPT mutation subjects, with higher standardized uptake value ratio in the R406W mutation associated with the presence of NFTs, and little non-specific binding. These results highlight that a positive 18F-MK-6240 tau-PET does not necessarily imply a diagnosis of Alzheimer's disease and point towards a potential use for 18F-MK-6240 as a biomarker in certain tauopathies beyond Alzheimer's, although further patient recruitment and autopsy studies will be necessary to determine clinical applicability.
Keywords: PET imaging; biomarkers; frontotemporal dementia.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Meeter LH, Kaat LD, Rohrer JD, van Swieten JC.. Imaging and fluid biomarkers in frontotemporal dementia. Nat Rev Neurol. 2017;13(7):406–419. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
