

Airway antibodies emerge according to COVID-19 severity and wane rapidly but reappear after SARS-CoV-2 vaccination
- PMID: 34665783
- PMCID: PMC8663786
- DOI: 10.1172/jci.insight.151463
Airway antibodies emerge according to COVID-19 severity and wane rapidly but reappear after SARS-CoV-2 vaccination
Abstract
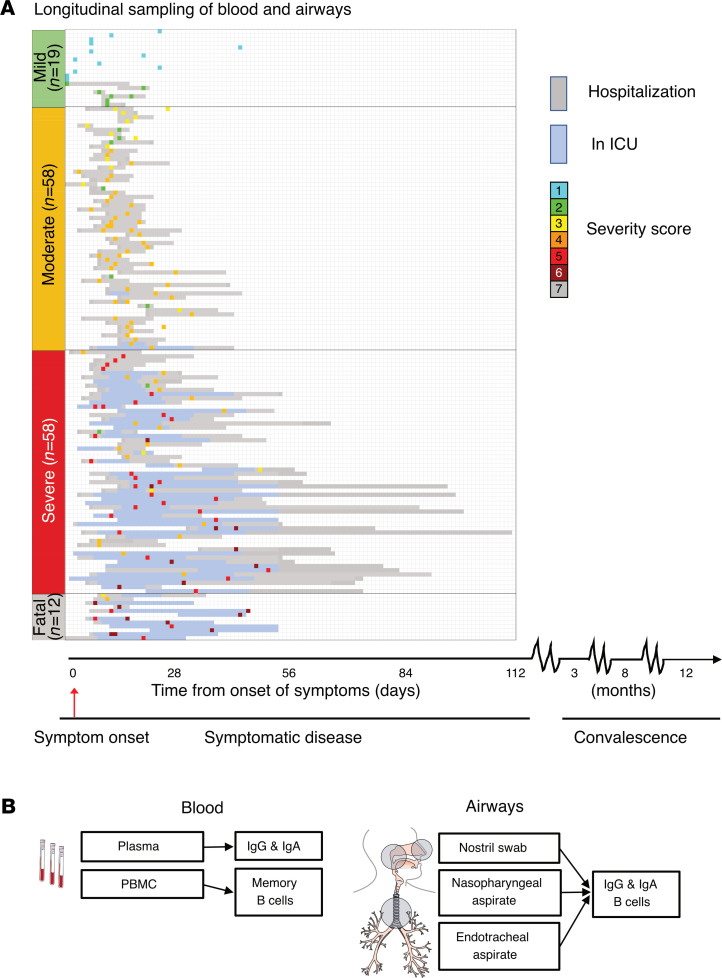
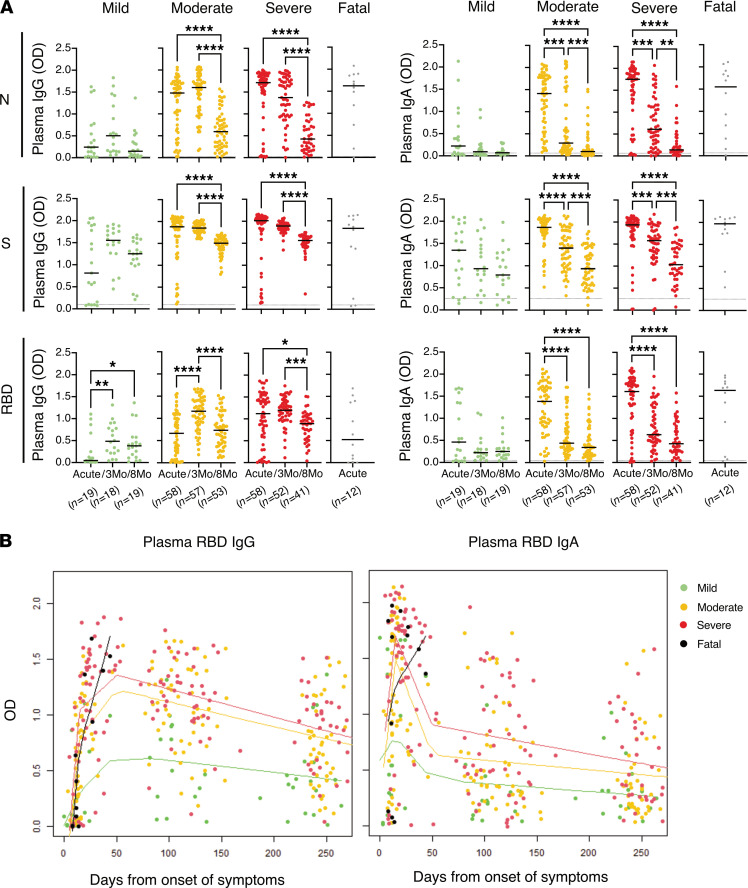
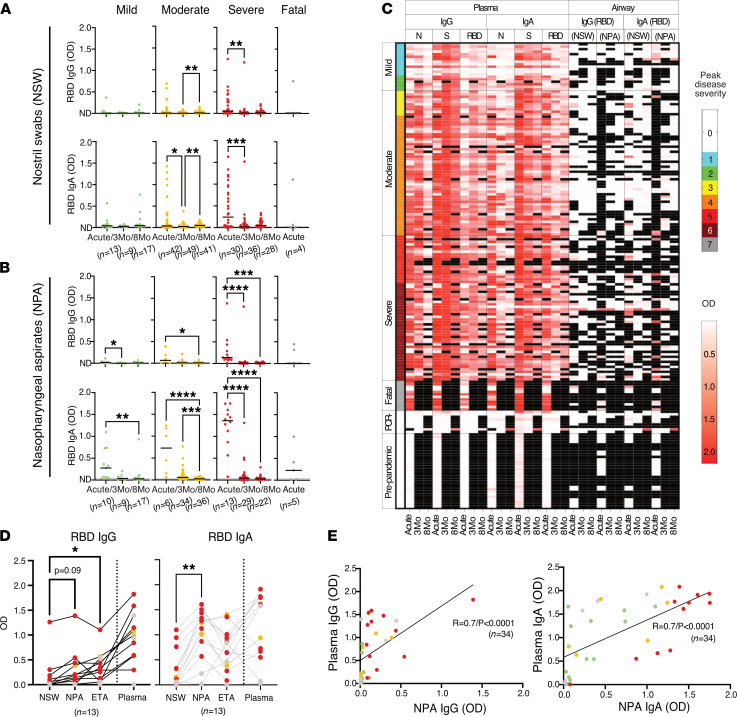
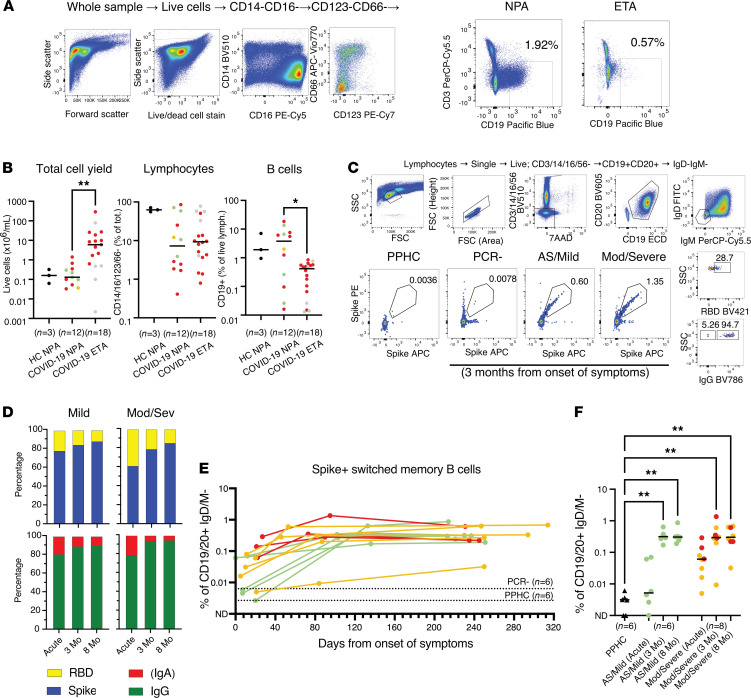
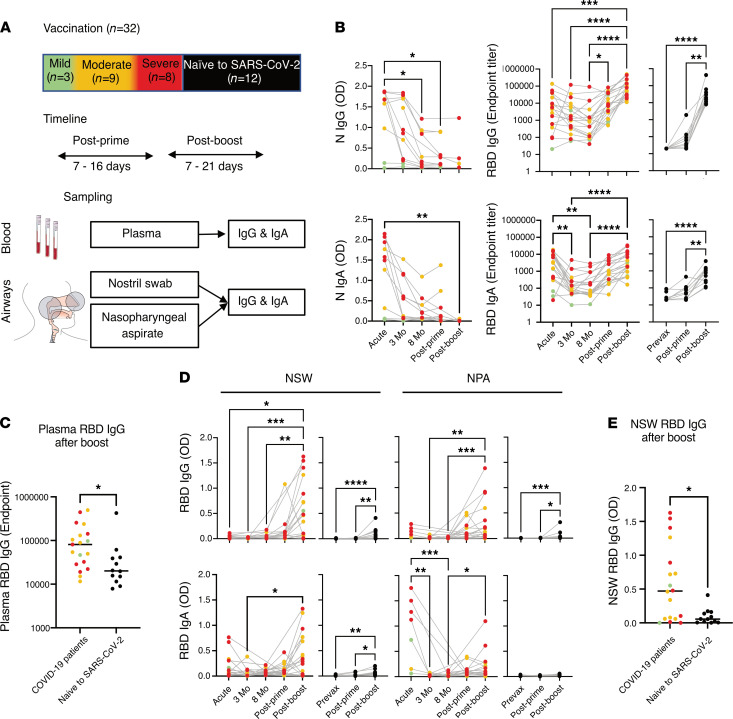
Understanding the presence and durability of antibodies against SARS-CoV-2 in the airways is required to provide insights into the ability of individuals to neutralize the virus locally and prevent viral spread. Here, we longitudinally assessed both systemic and airway immune responses upon SARS-CoV-2 infection in a clinically well-characterized cohort of 147 infected individuals representing the full spectrum of COVID-19 severity, from asymptomatic infection to fatal disease. In addition, we evaluated how SARS-CoV-2 vaccination influenced the antibody responses in a subset of these individuals during convalescence as compared with naive individuals. Not only systemic but also airway antibody responses correlated with the degree of COVID-19 disease severity. However, although systemic IgG levels were durable for up to 8 months, airway IgG and IgA declined significantly within 3 months. After vaccination, there was an increase in both systemic and airway antibodies, in particular IgG, often exceeding the levels found during acute disease. In contrast, naive individuals showed low airway antibodies after vaccination. In the former COVID-19 patients, airway antibody levels were significantly elevated after the boost vaccination, highlighting the importance of prime and boost vaccinations for previously infected individuals to obtain optimal mucosal protection.
Keywords: Adaptive immunity; COVID-19; Immunoglobulins; Immunology; Innate immunity.
Figures

Comment in
-
What's in the tissue? Immunology's new playground.Scand J Immunol. 2022 Feb;95(2):e13141. doi: 10.1111/sji.13141. Scand J Immunol. 2022. PMID: 35040510 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
