

Spinal Anesthesia with Targeted Sedation based on Bispectral Index Values Compared with General Anesthesia with Masked Bispectral Index Values to Reduce Delirium: The SHARP Randomized Controlled Trial
- PMID: 34666346
- PMCID: PMC8970606
- DOI: 10.1097/ALN.0000000000004015
Spinal Anesthesia with Targeted Sedation based on Bispectral Index Values Compared with General Anesthesia with Masked Bispectral Index Values to Reduce Delirium: The SHARP Randomized Controlled Trial
Abstract
Background: Reducing depth of anesthesia and anesthetic exposure may help prevent delirium, but trials have been conflicting. Most studies were conducted under general anesthesia or in cognitively impaired patients. It is unclear whether reducing depth of anesthesia beyond levels consistent with general anesthesia reduces delirium in cognitively intact patients. The authors' objective was to determine whether a bundled approach to reduce anesthetic agent exposure as determined by Bispectral Index (BIS) values (spinal anesthesia with targeted sedation based on BIS values) compared with general anesthesia (masked BIS) reduces delirium.
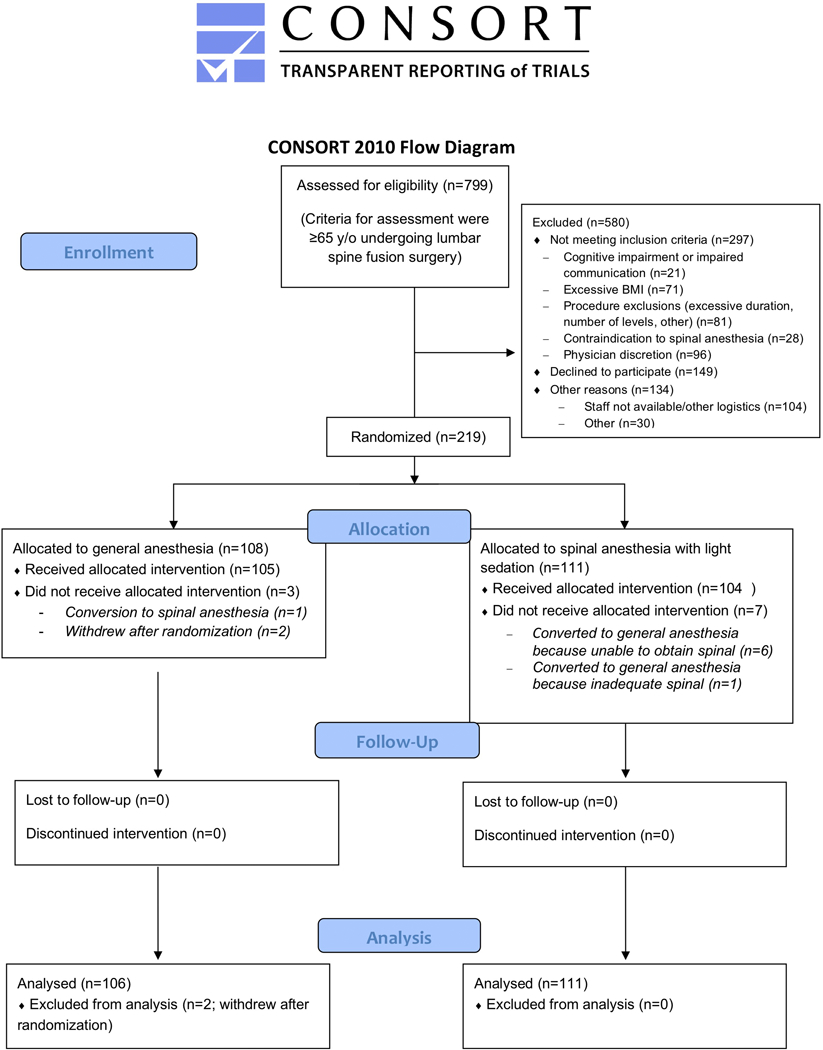
Methods: Important eligibility criteria for this parallel-arm randomized trial were patients 65 yr or greater undergoing lumbar spine fusion. The intervention group received spinal anesthesia with targeted sedation to BIS greater than 60 to 70. The control group received general anesthesia (masked BIS). The primary outcome was delirium using the Confusion Assessment Method daily through postoperative day 3, with blinded assessment.
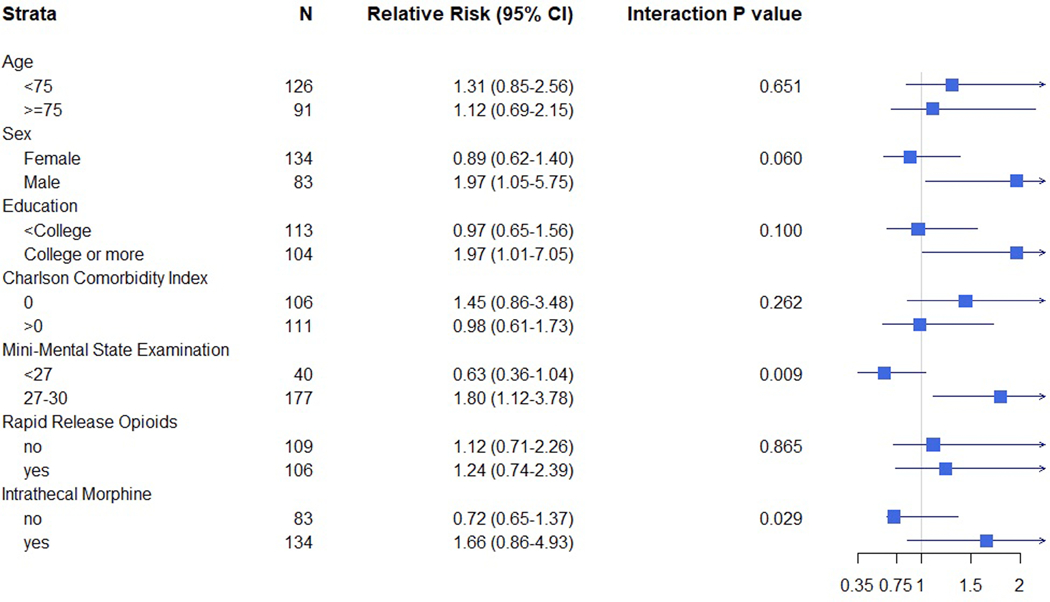
Results: The median age of 217 patients in the analysis was 72 (interquartile range, 69 to 77). The median BIS value in the spinal anesthesia with targeted sedation based on BIS values group was 62 (interquartile range, 53 to 70) and in the general anesthesia with masked BIS values group was 45 (interquartile range, 41 to 50; P < 0.001). Incident delirium was not different in the spinal anesthesia with targeted sedation based on BIS values group (25.2% [28 of 111] vs. the general anesthesia with masked BIS values group (18.9% [20 of 106]; P = 0.259; relative risk, 1.22 [95% CI, 0.85 to 1.76]). In prespecified subgroup analyses, the effect of anesthetic strategy differed according to the Mini-Mental State Examination, but not the Charlson Comorbidity Index or age. Two strokes occurred among patients receiving spinal anesthesia and one death among patients receiving general anesthesia.
Conclusions: Spinal anesthesia with targeted sedation based on BIS values compared with general anesthesia with masked BIS values did not reduce delirium after lumbar fusion.
Copyright © 2021, the American Society of Anesthesiologists. All Rights Reserved.
Conflict of interest statement
Conflicts of Interest
CB has consulted for and received grant funding from Medtronic
KJN has received grant funding from Hitachi Inc., and consulted for Merck Inc.
CH has received payment for advisory board membership from Medtronic Inc. (Minneapolis MN) and Edwards Lifesciences (Irvine CA). He serves on a Data Safety Monitoring Committee for Merck Inc. (Kenilworth NJ).
All other authors (CE, CL, LY, ME, YG, RS, DK, RC, NL, SC, ED FS, CD) have no other declaration of interests or conflicts of interests.
Figures
Comment in
-
Baseline Vulnerabilities May Play a Larger Role than Depth of Anesthesia or Sedation in Postoperative Delirium.Anesthesiology. 2021 Dec 1;135(6):940-942. doi: 10.1097/ALN.0000000000004039. Anesthesiology. 2021. PMID: 34731236 Free PMC article. No abstract available.
-
Targeting Depth of Anesthesia to Prevent Delirium: Comment.Anesthesiology. 2022 Jun 1;136(6):1045-1046. doi: 10.1097/ALN.0000000000004196. Anesthesiology. 2022. PMID: 35390114 No abstract available.
-
Targeting Depth of Anesthesia to Prevent Delirium: Comment.Anesthesiology. 2022 Jun 1;136(6):1046-1047. doi: 10.1097/ALN.0000000000004208. Anesthesiology. 2022. PMID: 35390117 No abstract available.
-
Targeting Depth of Anesthesia to Prevent Delirium: Reply.Anesthesiology. 2022 Jun 1;136(6):1047-1048. doi: 10.1097/ALN.0000000000004197. Anesthesiology. 2022. PMID: 35390124 No abstract available.
References
-
- American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. Postoperative delirium in older adults: Best practice statement from the american geriatrics society. J Am Coll Surg. 2015;220(2):136–48.e1. - PubMed
-
- Robinson TN, Raeburn CD, Tran ZV, Angles EM, Brenner LA, Moss M. Postoperative delirium in the elderly: Risk factors and outcomes. Ann Surg. 2009;249(1):173–178. - PubMed
-
- Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157–1165. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
