

Impact of clinical phenotypes on management and outcomes in European atrial fibrillation patients: a report from the ESC-EHRA EURObservational Research Programme in AF (EORP-AF) General Long-Term Registry
- PMID: 34666757
- PMCID: PMC8527730
- DOI: 10.1186/s12916-021-02120-3
Impact of clinical phenotypes on management and outcomes in European atrial fibrillation patients: a report from the ESC-EHRA EURObservational Research Programme in AF (EORP-AF) General Long-Term Registry
Abstract
Background: Epidemiological studies in atrial fibrillation (AF) illustrate that clinical complexity increase the risk of major adverse outcomes. We aimed to describe European AF patients' clinical phenotypes and analyse the differential clinical course.
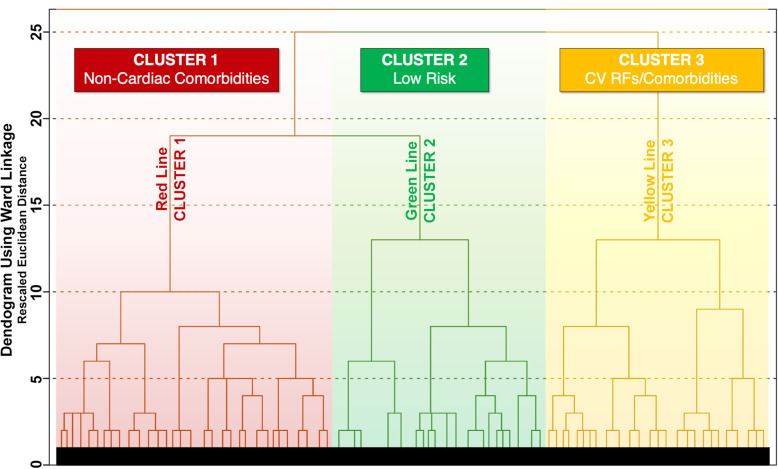
Methods: We performed a hierarchical cluster analysis based on Ward's Method and Squared Euclidean Distance using 22 clinical binary variables, identifying the optimal number of clusters. We investigated differences in clinical management, use of healthcare resources and outcomes in a cohort of European AF patients from a Europe-wide observational registry.
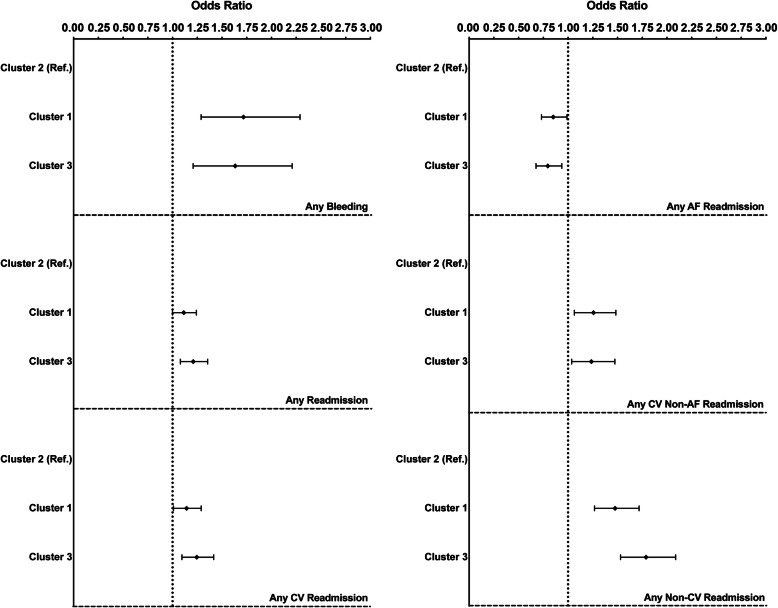
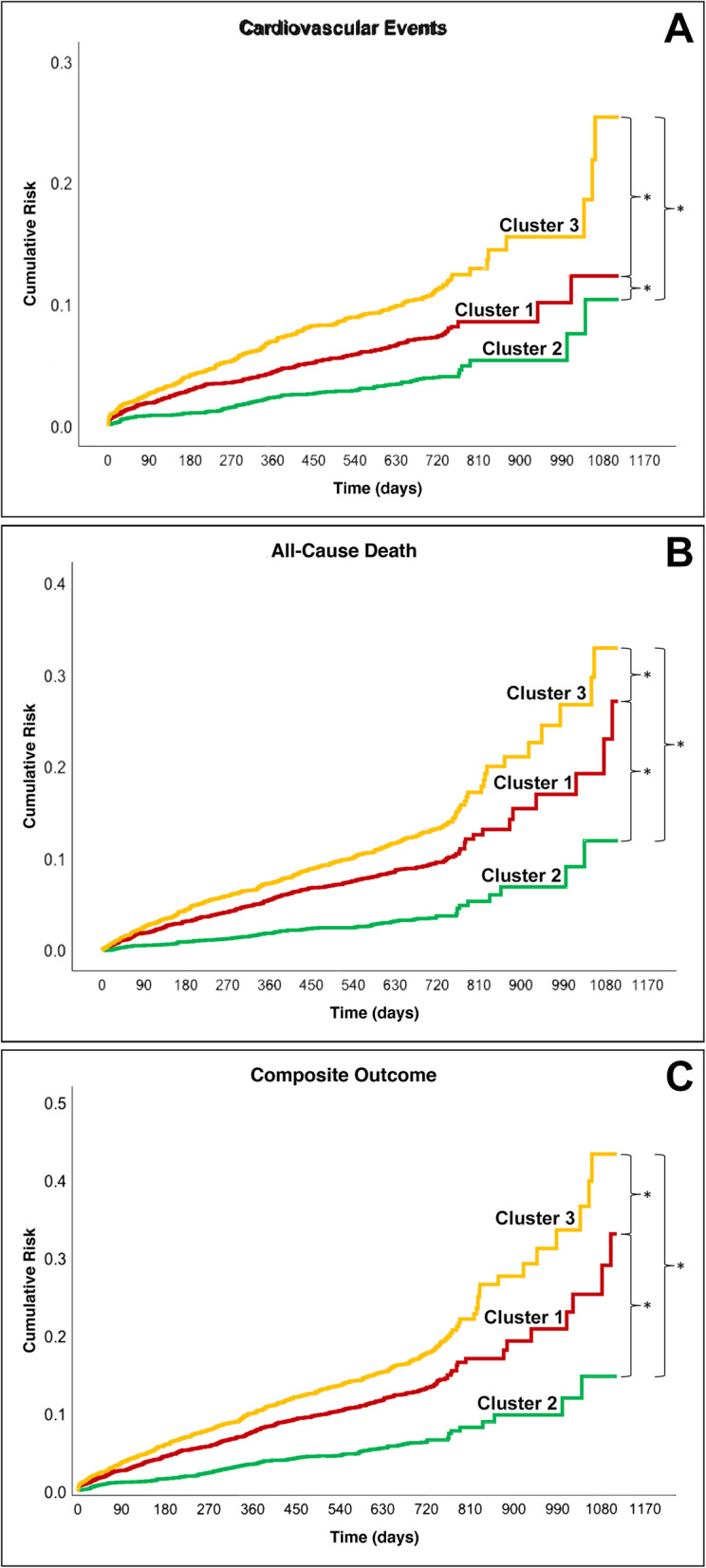
Results: A total of 9363 were available for this analysis. We identified three clusters: Cluster 1 (n = 3634; 38.8%) characterized by older patients and prevalent non-cardiac comorbidities; Cluster 2 (n = 2774; 29.6%) characterized by younger patients with low prevalence of comorbidities; Cluster 3 (n = 2955;31.6%) characterized by patients' prevalent cardiovascular risk factors/comorbidities. Over a mean follow-up of 22.5 months, Cluster 3 had the highest rate of cardiovascular events, all-cause death, and the composite outcome (combining the previous two) compared to Cluster 1 and Cluster 2 (all P < .001). An adjusted Cox regression showed that compared to Cluster 2, Cluster 3 (hazard ratio (HR) 2.87, 95% confidence interval (CI) 2.27-3.62; HR 3.42, 95%CI 2.72-4.31; HR 2.79, 95%CI 2.32-3.35), and Cluster 1 (HR 1.88, 95%CI 1.48-2.38; HR 2.50, 95%CI 1.98-3.15; HR 2.09, 95%CI 1.74-2.51) reported a higher risk for the three outcomes respectively.
Conclusions: In European AF patients, three main clusters were identified, differentiated by differential presence of comorbidities. Both non-cardiac and cardiac comorbidities clusters were found to be associated with an increased risk of major adverse outcomes.
Keywords: Atrial fibrillation; Clinical management; Clinical phenotypes; Cluster analysis; Major adverse outcomes.
© 2021. The Author(s).
Conflict of interest statement
DL has received investigator-initiated educational grants from Bristol-Myers Squibb (BMS), has been a speaker for Boehringer Ingelheim and BMS/Pfizer and has consulted for BMS, Boehringer Ingelheim and Daiichi Sankyo. LF has been a consultant or speaker for Bayer, BMS/Pfizer, Boehringer Ingelheim, Medtronic, Novartis; GB received small speaker’s fees from Medtronic, Boston, Boehringer Ingelheim and Bayer; GYHL has been a consultant and speaker for BMS/Pfizer, Boehringer Ingelheim and Daiichi Sankyo. No fees are directly received personally. All the disclosures happened outside the submitted work. All other authors have nothing to declare.
Figures
Similar articles
-
Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational Research Programme in AF General Long-Term Registry.BMC Med. 2022 Sep 2;20(1):326. doi: 10.1186/s12916-022-02526-7. BMC Med. 2022. PMID: 36056426 Free PMC article.
-
Optimal Medical Therapy for Heart Failure and Integrated Care in Patients With Atrial Fibrillation: A Report From the ESC-EHRA EORP Atrial Fibrillation Long-Term General Registry.J Am Heart Assoc. 2025 Jan 7;14(1):e030499. doi: 10.1161/JAHA.123.030499. Epub 2024 Dec 20. J Am Heart Assoc. 2025. PMID: 39704238 Free PMC article.
-
Relation of outcomes to ABC (Atrial Fibrillation Better Care) pathway adherent care in European patients with atrial fibrillation: an analysis from the ESC-EHRA EORP Atrial Fibrillation General Long-Term (AFGen LT) Registry.Europace. 2021 Feb 5;23(2):174-183. doi: 10.1093/europace/euaa274. Europace. 2021. PMID: 33006613
-
The Euro Heart Survey and EURObservational Research Programme (EORP) in atrial fibrillation registries: contribution to epidemiology, clinical management and therapy of atrial fibrillation patients over the last 20 years.Intern Emerg Med. 2020 Oct;15(7):1183-1192. doi: 10.1007/s11739-020-02405-0. Epub 2020 Jun 15. Intern Emerg Med. 2020. PMID: 32557091 Review.
-
Antithrombotic therapy in atrial fibrillation associated with valvular heart disease: a joint consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology Working Group on Thrombosis, endorsed by the ESC Working Group on Valvular Heart Disease, Cardiac Arrhythmia Society of Southern Africa (CASSA), Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), South African Heart (SA Heart) Association and Sociedad Latinoamericana de Estimulación Cardíaca y Electrofisiología (SOLEACE).Europace. 2017 Nov 1;19(11):1757-1758. doi: 10.1093/europace/eux240. Europace. 2017. PMID: 29096024 Review.
Cited by
-
Implications of Clinical Risk Phenotypes on the Management and Natural History of Atrial Fibrillation: A Report From the GLORIA-AF.J Am Heart Assoc. 2023 Oct 17;12(20):e030565. doi: 10.1161/JAHA.123.030565. Epub 2023 Oct 10. J Am Heart Assoc. 2023. PMID: 37815118 Free PMC article.
-
Impacts of Five Different Drying Methods on Volatile Organic Compounds in Mulberry Fruits.Foods. 2024 Nov 2;13(21):3514. doi: 10.3390/foods13213514. Foods. 2024. PMID: 39517298 Free PMC article.
-
Outcomes in Atrial Fibrillation Patients with Different Clinical Phenotypes: Insights from the French Population.J Clin Med. 2025 Feb 7;14(4):1044. doi: 10.3390/jcm14041044. J Clin Med. 2025. PMID: 40004575 Free PMC article.
-
Prognosis of Atrial Fibrillation with or without Comorbidities: Analysis of Younger Adults from a Nationwide Database.J Clin Med. 2022 Apr 1;11(7):1981. doi: 10.3390/jcm11071981. J Clin Med. 2022. PMID: 35407589 Free PMC article.
-
Risk of Death and Cardiovascular Events in Asian Patients With Atrial Fibrillation and Chronic Obstructive Pulmonary Disease: A Report From the Prospective APHRS Registry.J Am Heart Assoc. 2024 Apr 2;13(7):e032785. doi: 10.1161/JAHA.123.032785. Epub 2024 Mar 27. J Am Heart Assoc. 2024. PMID: 38533983 Free PMC article.
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, Fauchier L, Filippatos G, Kalman JM, la Meir M, Lane DA, Lebeau JP, Lettino M, Lip GYH, Pinto FJ, Thomas GN, Valgimigli M, van Gelder IC, van Putte BP, Watkins CL, ESC Scientific Document Group. Kirchhof P, Kühne M, Aboyans V, Ahlsson A, Balsam P, Bauersachs J, Benussi S, Brandes A, Braunschweig F, Camm AJ, Capodanno D, Casadei B, Conen D, Crijns HJGM, Delgado V, Dobrev D, Drexel H, Eckardt L, Fitzsimons D, Folliguet T, Gale CP, Gorenek B, Haeusler KG, Heidbuchel H, Iung B, Katus HA, Kotecha D, Landmesser U, Leclercq C, Lewis BS, Mascherbauer J, Merino JL, Merkely B, Mont L, Mueller C, Nagy KV, Oldgren J, Pavlović N, Pedretti RFE, Petersen SE, Piccini JP, Popescu BA, Pürerfellner H, Richter DJ, Roffi M, Rubboli A, Scherr D, Schnabel RB, Simpson IA, Shlyakhto E, Sinner MF, Steffel J, Sousa-Uva M, Suwalski P, Svetlosak M, Touyz RM, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, Fauchier L, Filippatos G, Kalman JM, la Meir M, Lane DA, Lebeau JP, Lettino M, Lip GYH, Pinto FJ, Neil Thomas G, Valgimigli M, van Gelder IC, Watkins CL, Delassi T, Sisakian HS, Scherr D, Chasnoits A, Pauw MD, Smajić E, Shalganov T, Avraamides P, Kautzner J, Gerdes C, Alaziz AA, Kampus P, Raatikainen P, Boveda S, Papiashvili G, Eckardt L, Vassilikos V, Csanádi Z, Arnar DO, Galvin J, Barsheshet A, Caldarola P, Rakisheva A, Bytyçi I, Kerimkulova A, Kalejs O, Njeim M, Puodziukynas A, Groben L, Sammut MA, Grosu A, Boskovic A, Moustaghfir A, Groot N, Poposka L, Anfinsen OG, Mitkowski PP, Cavaco DM, Siliste C, Mikhaylov EN, Bertelli L, Kojic D, Hatala R, Fras Z, Arribas F, Juhlin T, Sticherling C, Abid L, Atar I, Sychov O, Bates MGD, Zakirov NU. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2021;42(5):373–498. doi: 10.1093/eurheartj/ehaa612. - DOI - PubMed
-
- Proietti M, Laroche C, Nieuwlaat R, Crijns HJGM, Maggioni AP, Lane DA, Boriani G, Lip GYH, EORP-AF General Pilot Registry. Euro Heart Survey on AF Investigators Increased burden of comorbidities and risk of cardiovascular death in atrial fibrillation patients in Europe over ten years: a comparison between EORP-AF pilot and EHS-AF registries. Eur J Intern Med. 2018;55:28–34. doi: 10.1016/j.ejim.2018.05.016. - DOI - PubMed
