

Neoadjuvant Chemotherapy and Immunotherapy in Luminal B-like Breast Cancer: Results of the Phase II GIADA Trial
- PMID: 34667023
- PMCID: PMC9401542
- DOI: 10.1158/1078-0432.CCR-21-2260
Neoadjuvant Chemotherapy and Immunotherapy in Luminal B-like Breast Cancer: Results of the Phase II GIADA Trial
Abstract
Purpose: The role of immunotherapy in hormone receptor (HR)-positive, HER2-negative breast cancer is underexplored.
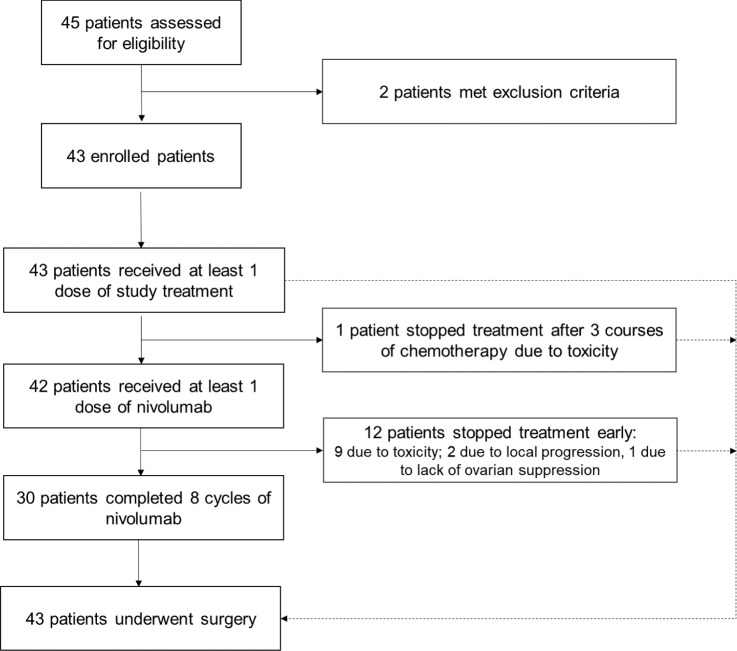
Patients and methods: The neoadjuvant phase II GIADA trial (NCT04659551, EUDRACT 2016-004665-10) enrolled stage II-IIIA premenopausal patients with Luminal B (LumB)-like breast cancer (HR-positive/HER2-negative, Ki67 ≥ 20%, and/or histologic grade 3). Patients received: three 21-day cycles of epirubicin/cyclophosphamide followed by eight 14-day cycles of nivolumab, triptorelin started concomitantly to chemotherapy, and exemestane started concomitantly to nivolumab. Primary endpoint was pathologic complete response (pCR; ypT0/is, ypN0).
Results: A pCR was achieved by 7/43 patients [16.3%; 95% confidence interval (CI), 7.4-34.9]; the rate of residual cancer burden class 0-I was 25.6%. pCR rate was significantly higher for patients with PAM50 Basal breast cancer (4/8, 50%) as compared with other subtypes (LumA 9.1%; LumB 8.3%; P = 0.017). Tumor-infiltrating lymphocytes (TIL), immune-related gene-expression signatures, and specific immune cell subpopulations by multiplex immunofluorescence were significantly associated with pCR. A combined score of Basal subtype and TILs had an AUC of 0.95 (95% CI, 0.89-1.00) for pCR prediction. According to multiplex immunofluorescence, a switch to a more immune-activated tumor microenvironment occurred following exposure to anthracyclines. Most common grade ≥3 treatment-related adverse events (AE) during nivolumab were γ-glutamyltransferase (16.7%), alanine aminotransferase (16.7%), and aspartate aminotransferase (9.5%) increase. Most common immune-related AEs were endocrinopathies (all grades 1-2; including adrenal insufficiency, n = 1).
Conclusions: Luminal B-like breast cancers with a Basal molecular subtype and/or a state of immune activation may respond to sequential anthracyclines and anti-PD-1. Our data generate hypotheses that, if validated, could guide immunotherapy development in this context.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures


Comment on
-
Selected Articles from This Issue.Clin Cancer Res. 2022 Jan 15;28(2):247. doi: 10.1158/1078-0432.CCR-28-2-HI. Clin Cancer Res. 2022. PMID: 35045957 No abstract available.
References
-
- Cardoso F, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rubio IT, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2019;30:1194–220. - PubMed
-
- Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014;384:164–72. - PubMed
-
- von Minckwitz G, Untch M, Blohmer J-U, Costa SD, Eidtmann H, Fasching PA, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 2012;30:1796–804. - PubMed
-
- Gianni L, Mansutti M, Anton A, Calvo L, Bisagni G, Bermejo B, et al. Comparing neoadjuvant nab-paclitaxel vs paclitaxel both followed by anthracycline regimens in women with ERBB2/HER2-negative breast cancer—the evaluating treatment with neoadjuvant abraxane (ETNA) trial: a randomized phase 3 clinical trial. JAMA Oncol 2018;4:302–8. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
