

Health care costs of hospitalization of young children for respiratory syncytial virus infections: a population-based matched cohort study
- PMID: 34667075
- PMCID: PMC8526091
- DOI: 10.9778/cmajo.20200219
Health care costs of hospitalization of young children for respiratory syncytial virus infections: a population-based matched cohort study
Abstract
Background: Respiratory syncytial virus (RSV) infection poses a substantial clinical burden among infants and young children. We sought to determine the health care costs of hospitalizations attributable to RSV in Ontario, Canada, from the health care payer perspective.
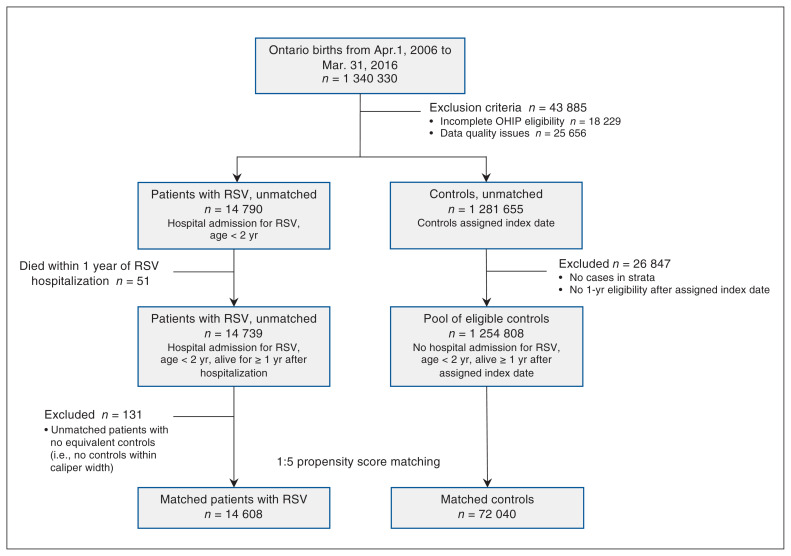
Methods: For this population-based matched cohort study, we identified children younger than 24 months who were or were not hospitalized with RSV infections in 2006-2016. We performed a cost-of-illness analysis using linked administrative health data, with subjects stratified by gestational age and congenital heart disease, and propensity score-matched on established risk factors. The primary outcome was attributable health care costs per patient, reflecting the difference in direct medical costs between the groups, calculated to 12 months postdischarge in 2020 Canadian dollars.
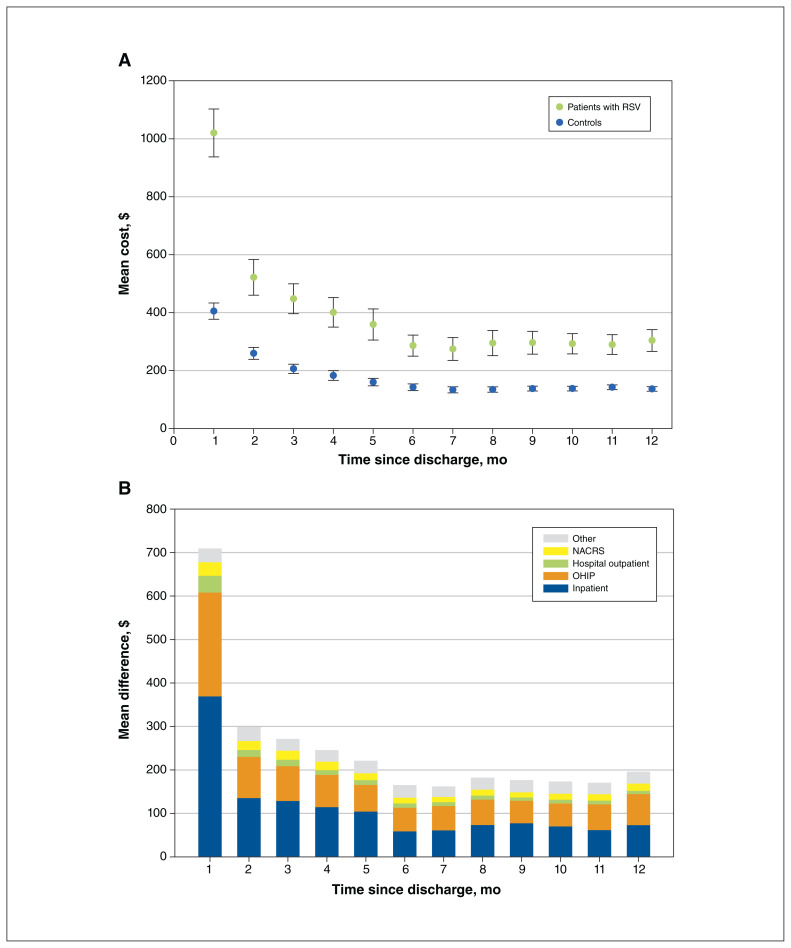
Results: We identified 14 608 RSV-infected children, matched to 72 040 controls. The adjusted attributable cost of hospitalized RSV was $134 931 900 over 10 years, or $9240 per patient (95% confidence interval [CI] $8790-$9690). Health care costs escalated 3 days before hospitalization, and persisted up to 12 months after discharge. Increased costs were associated with major comorbidities, but not extreme premature birth. The highest mean attributable cost per patient was in the presence of hemodynamically significant heart disease ($60 110, 95% CI $26 700-$93 060). Infants born at 36-43 weeks' gestation constituted the greatest overall cost burden at $117 886 720.
Interpretation: Although the greatest direct medical costs per patient hospitalized with RSV infection are among children with cardiac disease, the greatest overall cost burden is from children born at or near term, who are not targeted by current prophylaxis strategies. The substantial attributable health care costs of RSV can inform cost-effectiveness analyses of novel RSV vaccines and prioritization of health care resources.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Krista Lanctot reports grants from AbbVie Canada and stock from Highmark Interactive, outside the submitted work. J. Dayre McNally reports funding from the Canadian Institutes of Health Research, outside the submitted work. No other competing interests were declared.
Figures
References
-
- Buchan SA, Chung H, Karnauchow T, et al. Characteristics and outcomes of young children hospitalized with laboratory-confirmed influenza or respiratory syncytial virus in Ontario, Canada, 2009–2014. Pediatr Infect Dis J. 2019;38:362–9. - PubMed
-
- Shi T, McAllister DA, O’Brien KL, et al. RSV Global Epidemiology Network. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390:946–58. - PMC - PubMed
-
- Hall CB, Weinberg GA, Blumkin AK, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. 2013;132:e341–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical