

Assessing the utility and accuracy of ICD10-CM non-traumatic subarachnoid hemorrhage codes for intracranial aneurysm research
- PMID: 34667877
- PMCID: PMC8512725
- DOI: 10.1002/lrh2.10257
Assessing the utility and accuracy of ICD10-CM non-traumatic subarachnoid hemorrhage codes for intracranial aneurysm research
Abstract
Background: The 10th revision of International Classification of Disease, Clinical Modification (ICD10-CM) increased the number of codes to identify non-traumatic subarachnoid hemorrhage from 1 to 22. ICD10-CM codes are able to specify the location of aneurysms causing subarachnoid hemorrhage (aSAH); however, it is not clear how frequently or accurately these codes are being used in practice.
Objective: To systematically evaluate the usage and accuracy of location-specific ICD10-CM codes for aSAH.
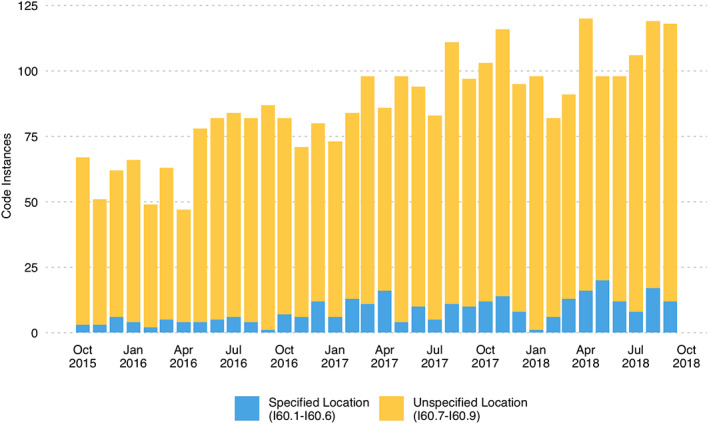
Methods: We extracted all uses of ICD10-CM codes for non-traumatic subarachnoid hemorrhage (I60.x) during the first 3 years following the implementation of ICD10-CM from the billing module of the electronic health record (EHR) for UCHealth. For those codes that specified aSAH location (I60.0-I60.6), EHR documentation was reviewed to determine whether there was an active aSAH, any patient history of aSAH, or unruptured intracranial aneurysm/s and the locations of those outcomes.
Results: Between 1 October 2015 and 30 September 2018, there were 3119 instances of non-traumatic subarachnoid hemorrhage ICD10-CM codes (I60.00-I60.9), of which 297 (9.5%) code instances identified aSAH location (I60.0-I60.6). The usage of location-specific codes increased from 5.7% in 2015 to 11.2% in 2018. These codes accurately identified current aSAH (64%), any patient history of aSAH (84%), and any patient history of intracranial aneurysm (87%). The accuracy of identified outcome location was 53% in current aSAH, 72% for any history of aSAH, and 76% for any history of an intracranial aneurysm.
Conclusions: Researchers should use ICD10-CM codes with caution when attempting to detect active aSAH and/or aneurysm location.
Keywords: administrative databases; electronic health records; intracranial aneurysm; subarachnoid hemorrhage.
© 2021 The Authors. Learning Health Systems published by Wiley Periodicals LLC on behalf of the University of Michigan.
Conflict of interest statement
None.
Figures



References
-
- Vernooij MW, Ikram MA, Tanghe HL, et al. Incidental findings on brain MRI in the general population. N Engl J Med. 2007;357(18):1821‐1828. - PubMed
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta‐analysis. Lancet Neurol. 2011;10(7):626‐636. - PubMed
-
- Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998;29(1):251‐256. - PubMed
-
- Hop JW, Rinkel GJE, Algra A, van Gijn J. Case‐fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke. 1997;28(3):660–664. - PubMed
-
- Molyneux A, Kerr R, Group ISAT (isat) C . International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomized trial. J Stroke Cerebrovasc Dis. 2002;11(6):304‐314. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
