

Mastication after craniotomy: pilot assessment of postoperative oral health-related quality of life
- PMID: 34668078
- PMCID: PMC9061666
- DOI: 10.1007/s00701-021-05020-w
Mastication after craniotomy: pilot assessment of postoperative oral health-related quality of life
Abstract
Background: Neurosurgical approaches to the brain often require the mobilization of the temporal muscle. Many patients complain of postoperative pain, atrophy, reduced mouth opening, and masticatory problems. Although the pterional, frontolateral-extended-pterional, and temporal craniotomies are the most frequently used approaches in neurosurgery, a systematic assessment of the postoperative oral health-related quality of life has never been performed so far. This study evaluates the oral health-related quality of life of patients after pterional, frontolateral-extended-pterional, or temporal craniotomy using a validated and standardized dental questionnaire, compares the results with the normal values of the general population, and investigates whether this questionnaire is sensitive to changes caused by surgical manipulation of the temporal muscle.
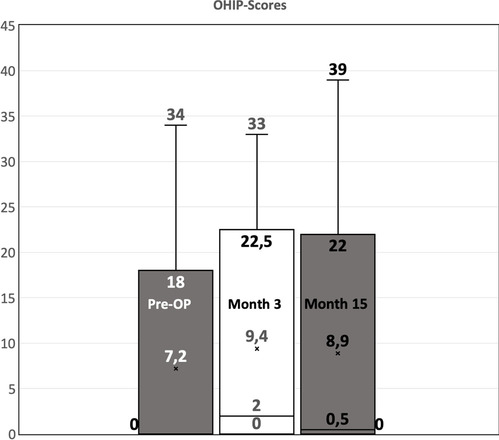
Methods: The "Oral Health Impact Profile" (OHIP14) is a validated questionnaire to assess the oral health-related quality of life. It asks the patients to assess their oral health situation within the past 7 days in 14 questions. Possible answers range from 0 (never) to 4 (very often). Sixty patients with benign intracranial processes operated through a lateral cranial approach were included. The questionnaire was answered before surgery (baseline) and 3 months and 15 months after surgery.
Results: Overall, postoperative OHIP scores increase significantly after 3 months and decrease after 15 months, but not to preoperative values. No factors can be identified which show a considerable relationship with the postoperative OHIP score.
Conclusions: Postoperative impairment of mouth opening and pain during mastication can be observed 3 to 15 months after surgery and sometimes cause feedback from patients and their dentists. However, in line with existing literature, these complaints decrease with time. The study shows that the OHIP questionnaire is sensitive to changes caused by surgical manipulation of the temporal muscle and can therefore be used to investigate the influence of surgical techniques on postoperative complaints. Postoperatively, patients show worse OHIP scores than the general population, demonstrating that neurosurgical cranial approaches negatively influence the patient's oral health-related wellbeing. Larger studies using the OHIP questionnaire should evaluate if postoperative physical therapy, speech therapy, or specialized rehabilitation devices can improve the masticatory impairment after craniotomy.
Trial registration: Clinical trial register: DRKS00011096.
Keywords: Atrophy; Craniotomy; OHIP; QoL; Quality of life; Temporal muscle.
© 2021. The Author(s).
Figures

References
-
- Andrade FCD, Jr, Andrade FCD, Araujo Filho CMD, Carcagnolo Filho J. Dysfunction of the temporalis muscle after pterional craniotomy for intracranial aneurysms: comparative, prospective and randomized study of one flap versus two flaps dieresis. Arq Neuro-Psiquiatr. 1998;56(2):200–205. doi: 10.1590/S0004-282X1998000200006. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
