

Change in central nervous system-active medication use following fall-related injury in older adults
- PMID: 34668191
- PMCID: PMC8742750
- DOI: 10.1111/jgs.17508
Change in central nervous system-active medication use following fall-related injury in older adults
Abstract
Background: Central nervous system (CNS)-active medication use is an important modifiable risk factor for falls in older adults. A fall-related injury should prompt providers to evaluate and reduce CNS-active medications to prevent recurrent falls. We evaluated change in CNS-active medications up to 12 months following a fall-related injury in community-dwelling older adults compared with a matched cohort without fall-related injury.
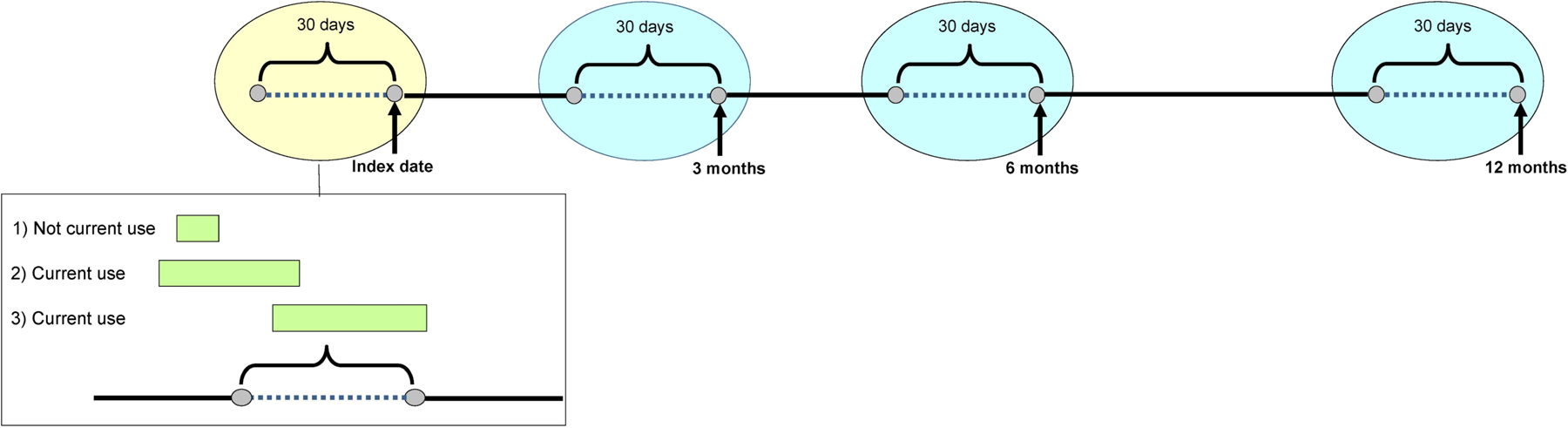
Methods: Participants were from the Adult Changes in Thought study conducted at Kaiser Permanente Washington. Fall-related injury codes between 1994 and 2014 defined index encounters in participants with no evidence of such injuries in the preceding year. We matched each fall-related injury index encounter with up to five randomly selected clinical encounters from participants without injury. Using automated pharmacy data, we estimated the average change in CNS-active medication use at 3, 6, and 12 months post-index according to the presence or absence of CNS-active medication use before index.
Results: One thousand five hundred sixteen participants with fall-related injury index encounters (449 CNS-active users, 1067 nonusers) were matched to 7014 index encounters from people without fall-related injuries (1751 users, 5236 nonusers). Among CNS-active users at the index encounter, those with fall-related injury had an average decrease in standard daily doses (SDDs) at 12 months (-0.43; 95% CI: -0.63 to -0.23), and those without injury had a greater (p = 0.047) average decrease (-0.66; 95% CI: -0.78 to -0.55). Among nonusers at index, those with fall-related injury had a smaller increase than those without injury (+0.17, 95% CI: +0.13 to +0.21, vs. +0.24, 95% CI: +0.20 to +0.28, p = 0.005).
Conclusions: The differences in CNS-active medication use change over 12 months between those with and without fall-related injury were small and unlikely to be clinically significant. These results suggest that fall risk-increasing drug use is not reduced following a fall-related injury, thus opportunities exist to reduce CNS-active medications, a potentially modifiable risk factor for falls.
Keywords: fall-related injury; medications; older adults.
© 2021 The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Olfson M, King M, Schoenbaum M. Benzodiazepine use in the United States. JAMA psychiatry. 2015;72(2):136–142. - PubMed
-
- Bergen G, Stevens MR, Burns ER. Falls and Fall Injuries Among Adults Aged >/=65 Years - United States, 2014. MMWR Morbidity and mortality weekly report. 2016;65(37):993–998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
