

Neurological autoimmune diseases following vaccinations against SARS-CoV-2: a case series
- PMID: 34668274
- PMCID: PMC8652629
- DOI: 10.1111/ene.15147
Neurological autoimmune diseases following vaccinations against SARS-CoV-2: a case series
Abstract
Background and purpose: Population-based studies suggest that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines may trigger immune-mediated thrombotic thrombocytopenia (VITT) raising concerns for other autoimmune responses. The aim was to characterize neurological autoimmunity after SARS-CoV-2 vaccinations.
Methods: In this single-centre prospective case study patients with neurological autoimmunity in temporal association (≤6 weeks) with SARS-CoV-2 vaccinations and without other triggers are reported. Clinical, laboratory and imaging data were collected with a median follow-up of 49 days.
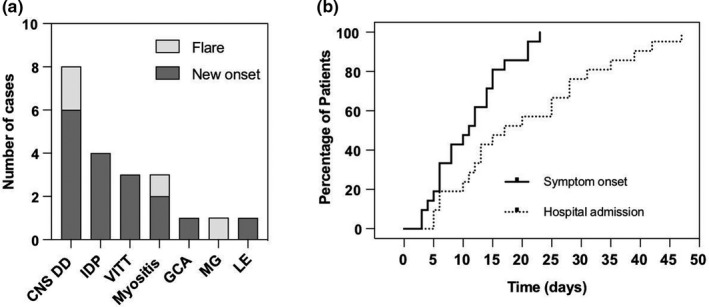
Results: In the study period 232,603 inhabitants from the main catchment area of our hospital (Rhein-Neckar-Kreis, county) received SARS-CoV-2 vaccinations. Twenty-one cases (new onset n = 17, flares n = 4) diagnosed a median of 11 days (range 3-23) following SARS-CoV-2 vaccinations (BNT162b2 n = 12, ChAdOx1 n = 8, mRNA-1273 n = 1) were identified. Cases included VITT with cerebral venous sinus thrombosis (n = 3), central nervous system demyelinating diseases (n = 8), inflammatory peripheral neuropathies (n = 4), myositis (n = 3), myasthenia (n = 1), limbic encephalitis (n = 1) and giant cell arteritis (n = 1). Patients were predominantly female (ratio 3.2:1) and the median age at diagnosis was 50 years (range 22-86). Therapy included administration of steroids (n = 15), intravenous immunoglobulins in patients with Guillain-Barré syndrome or VITT (n = 4), plasma exchange in cases unresponsive to steroids (n = 3) and anticoagulation in VITT. Outcomes were favourable with partial and complete remissions achieved in 71% and 24%, respectively. Two patients received their second vaccination without further aggravation of autoimmune symptoms under low-dose immunosuppressants.
Conclusions: In this study various neurological autoimmune disorders encountered following SARS-CoV-2 vaccinations are characterized. Given the assumed low incidence and mostly favourable outcome of autoimmune responses, the benefits of vaccinations outweigh the comparatively small risks.
Keywords: COVID-19; Guillain-Barré syndrome; autoimmune; cerebral venous sinus thrombosis; multiple sclerosis; myelitis; myositis.
© 2021 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
None declared.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
