

Classifying Esophageal Motility by FLIP Panometry: A Study of 722 Subjects With Manometry
- PMID: 34668487
- PMCID: PMC8825704
- DOI: 10.14309/ajg.0000000000001532
Classifying Esophageal Motility by FLIP Panometry: A Study of 722 Subjects With Manometry
Abstract
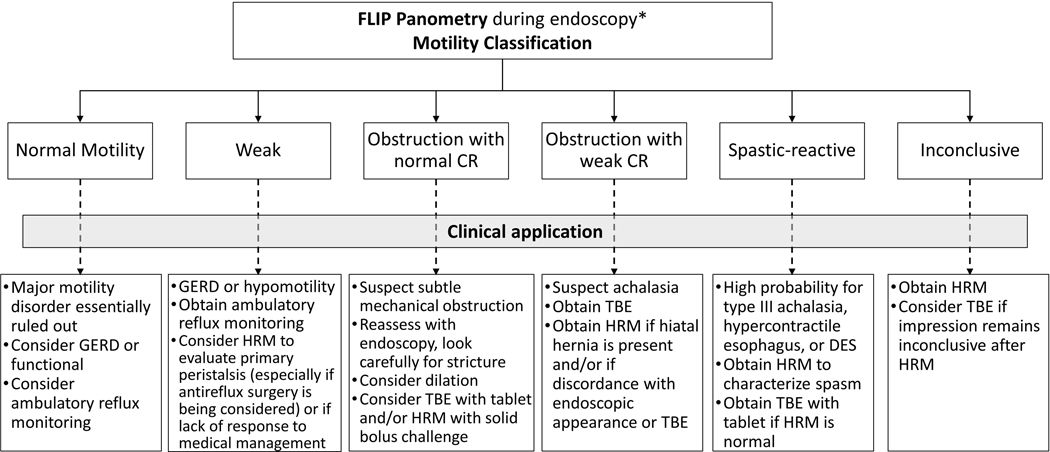
Introduction: Functional luminal imaging probe (FLIP) panometry can evaluate esophageal motility in response to sustained esophageal distension at the time of sedated endoscopy. This study aimed to describe a classification of esophageal motility using FLIP panometry and evaluate it against high-resolution manometry (HRM) and Chicago Classification v4.0 (CCv4.0).
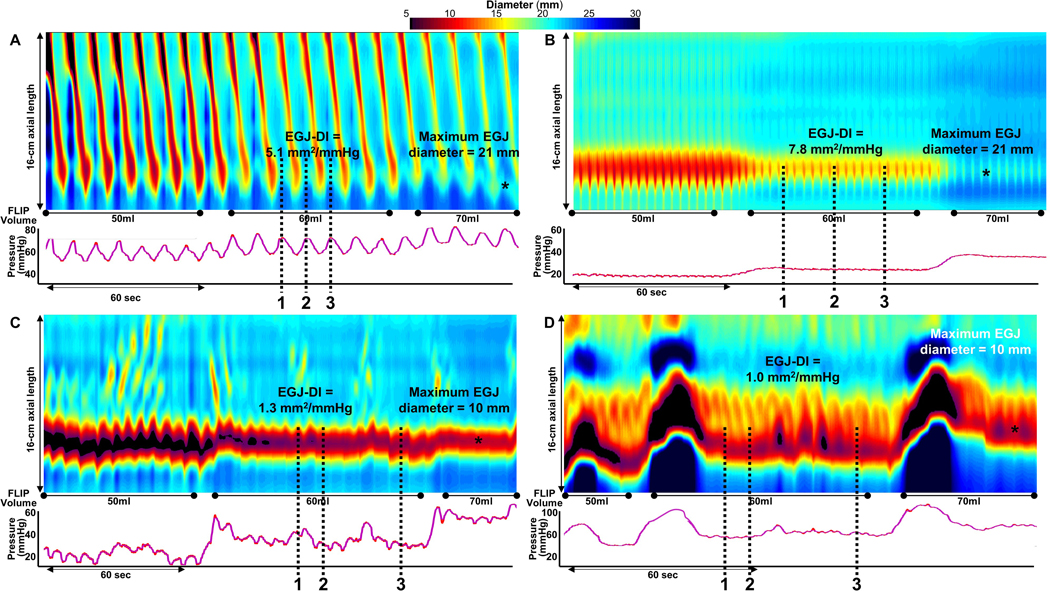
Methods: Five hundred thirty-nine adult patients who completed FLIP and HRM with a conclusive CCv4.0 diagnosis were included in the primary analysis. Thirty-five asymptomatic volunteers ("controls") and 148 patients with an inconclusive CCv4.0 diagnosis or systemic sclerosis were also described. Esophagogastric junction (EGJ) opening and the contractile response (CR) to distension (i.e., secondary peristalsis) were evaluated with a 16-cm FLIP during sedated endoscopy and analyzed using a customized software program. HRM was classified according to CCv4.0.
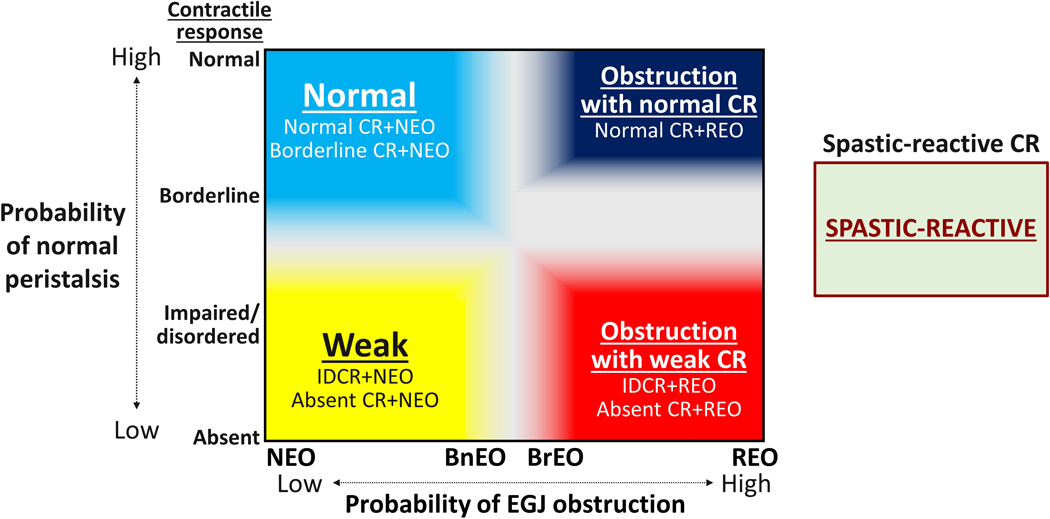
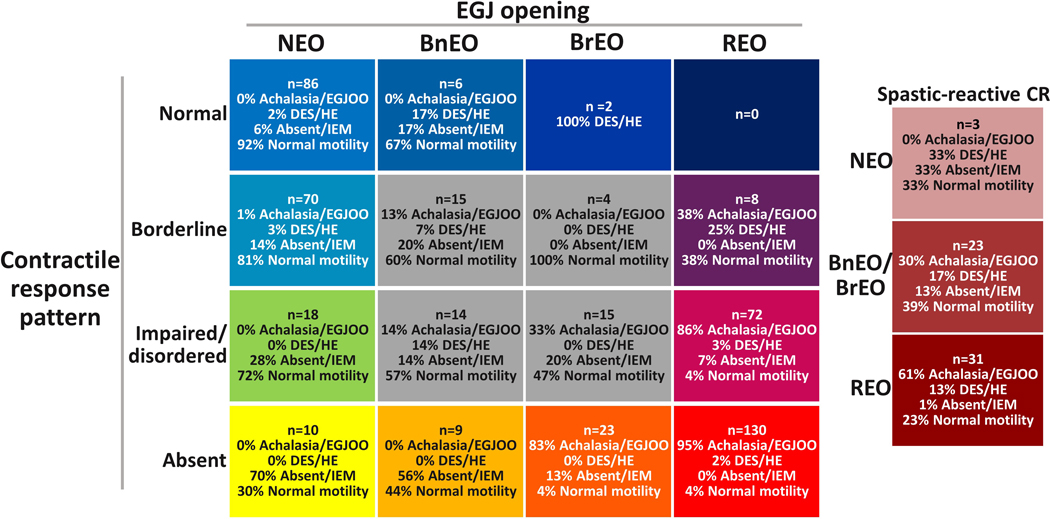
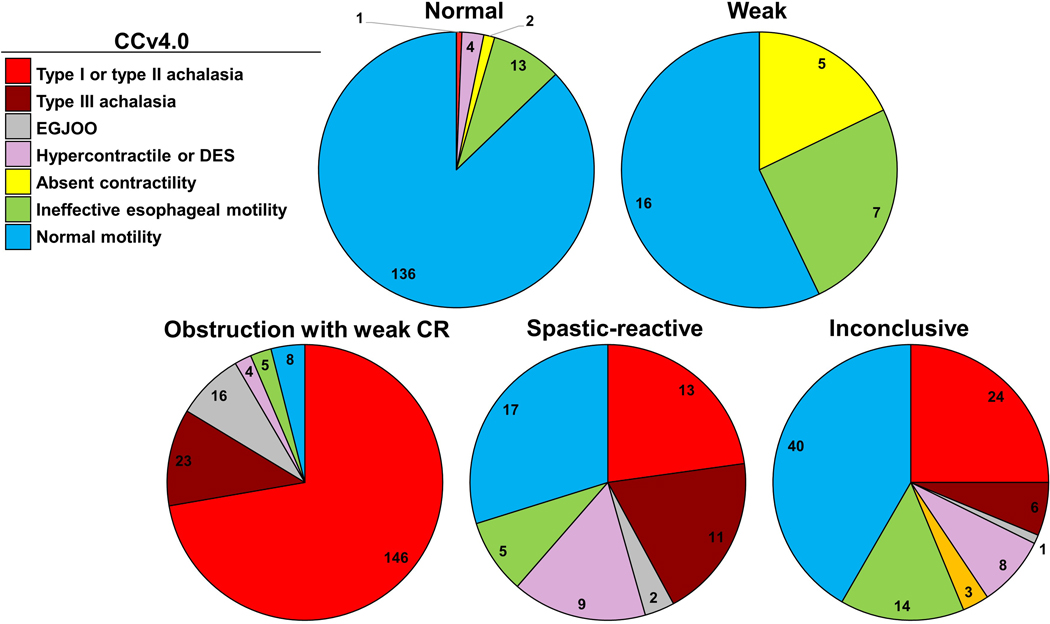
Results: In the primary analysis, 156 patients (29%) had normal motility on FLIP panometry, defined by normal EGJ opening and a normal or borderline CR; 95% of these patients had normal motility or ineffective esophageal motility on HRM. Two hundred two patients (37%) had obstruction with weak CR, defined as reduced EGJ opening and absent CR or impaired/disordered CR, on FLIP panometry; 92% of these patients had a disorder of EGJ outflow per CCv4.0.
Discussion: Classifying esophageal motility in response to sustained distension with FLIP panometry parallels the swallow-associated motility evaluation provided with HRM and CCv4.0. Thus, FLIP panometry serves as a well-tolerated method that can complement, or in some cases be an alternative to HRM, for evaluating esophageal motility disorders.
Copyright © 2021 by The American College of Gastroenterology.
Figures
Similar articles
-
Validation of Clinically Relevant Thresholds of Esophagogastric Junction Obstruction Using FLIP Panometry.Clin Gastroenterol Hepatol. 2022 Jun;20(6):e1250-e1262. doi: 10.1016/j.cgh.2021.06.040. Epub 2021 Jun 30. Clin Gastroenterol Hepatol. 2022. PMID: 34216821 Free PMC article.
-
Validation of secondary peristalsis classification using FLIP panometry in 741 subjects undergoing manometry.Neurogastroenterol Motil. 2022 Jan;34(1):e14192. doi: 10.1111/nmo.14192. Epub 2021 Jun 13. Neurogastroenterol Motil. 2022. PMID: 34120383 Free PMC article.
-
Discriminating "impaired" from "disordered" contractile response on FLIP panometry by utilizing pressure measurement.Neurogastroenterol Motil. 2024 Jul;36(7):e14818. doi: 10.1111/nmo.14818. Epub 2024 May 19. Neurogastroenterol Motil. 2024. PMID: 38764235
-
Functional luminal imaging probe in the evaluation of esophago-gastric junction outflow obstruction.Curr Opin Gastroenterol. 2022 Jul 1;38(4):388-394. doi: 10.1097/MOG.0000000000000843. Curr Opin Gastroenterol. 2022. PMID: 35762698 Review.
-
A Standardized Approach to Performing and Interpreting Functional Lumen Imaging Probe Panometry for Esophageal Motility Disorders: The Dallas Consensus.Gastroenterology. 2025 Jun;168(6):1114-1127.e5. doi: 10.1053/j.gastro.2025.01.234. Epub 2025 Feb 4. Gastroenterology. 2025. PMID: 39914779
Cited by
-
Identifying spastic variant of type II achalasia after treatment with high-resolution manometry and FLIP Panometry.Neurogastroenterol Motil. 2023 Jul;35(7):e14552. doi: 10.1111/nmo.14552. Epub 2023 Feb 21. Neurogastroenterol Motil. 2023. PMID: 36807659 Free PMC article.
-
Impedance planimetry and panometry (EndoFLIP™) can replace manometry in preoperative anti-reflux surgery assessment.Surg Endosc. 2024 Jan;38(1):339-347. doi: 10.1007/s00464-023-10419-w. Epub 2023 Sep 28. Surg Endosc. 2024. PMID: 37770608
-
Opioid-induced Esophageal Dysfunction Masquerading as Type I Achalasia.J Neurogastroenterol Motil. 2024 Oct 30;30(4):517-519. doi: 10.5056/jnm24088. J Neurogastroenterol Motil. 2024. PMID: 39397629 Free PMC article. No abstract available.
-
Concomitant Achalasia and Barrett's Esophagus: A Rare Coincidence.ACG Case Rep J. 2024 Apr 27;11(5):e01341. doi: 10.14309/crj.0000000000001341. eCollection 2024 May. ACG Case Rep J. 2024. PMID: 38690567 Free PMC article.
-
Peristaltic regimes in esophageal transport.Biomech Model Mechanobiol. 2023 Feb;22(1):23-41. doi: 10.1007/s10237-022-01625-x. Epub 2022 Nov 9. Biomech Model Mechanobiol. 2023. PMID: 36352039 Free PMC article.
References
-
- Pandolfino JE, Ghosh SK, Rice J, Clarke JO, Kwiatek MA, Kahrilas PJ. Classifying esophageal motility by pressure topography characteristics: a study of 400 patients and 75 controls. Am J Gastroenterol. 2008;103(1):27–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
