

Risk Factors for Being Seronegative following SARS-CoV-2 Infection in a Large Cohort of Health Care Workers in Denmark
- PMID: 34668738
- PMCID: PMC8528102
- DOI: 10.1128/Spectrum.00904-21
Risk Factors for Being Seronegative following SARS-CoV-2 Infection in a Large Cohort of Health Care Workers in Denmark
Abstract
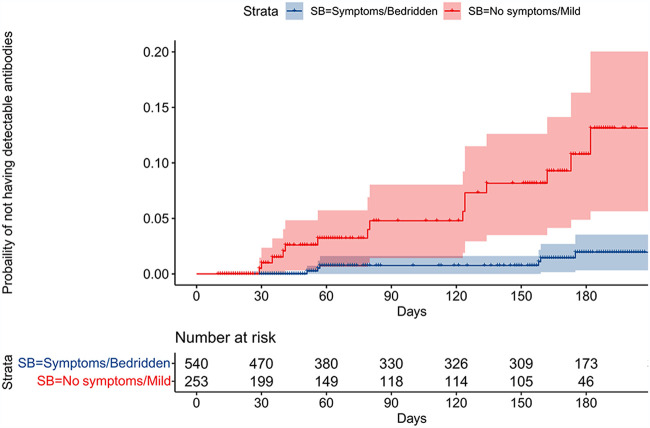
Most individuals seroconvert after infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but being seronegative is observed in 1 to 9%. We aimed to investigate the risk factors associated with being seronegative following PCR-confirmed SARS-CoV-2 infection. In a prospective cohort study, we screened health care workers (HCW) in the Capital Region of Denmark for SARS-CoV-2 antibodies. We performed three rounds of screening from April to October 2020 using an enzyme-linked immunosorbent assay (ELISA) method targeting SARS-CoV-2 total antibodies. Data on all participants' PCR for SARS-CoV-2 RNA were captured from national registries. The Kaplan-Meier method and Cox proportional hazards models were applied to investigate the probability of being seronegative and the related risk factors, respectively. Of 36,583 HCW, 866 (2.4%) had a positive PCR before or during the study period. The median (interquartile range [IQR]) age of 866 HCW was 42 (31 to 53) years, and 666 (77%) were female. After a median of 132 (range, 35 to 180) days, 21 (2.4%) of 866 were seronegative. In a multivariable model, independent risk factors for being seronegative were self-reported asymptomatic or mild infection hazard ratio (HR) of 6.6 (95% confidence interval [CI], 2.6 to 17; P < 0.001) and body mass index (BMI) of ≥30, HR 3.1 (95% CI, 1.1 to 8.8; P = 0.039). Only a few (2.4%) HCW were not seropositive. Asymptomatic or mild infection as well as a BMI above 30 were associated with being seronegative. Since the presence of antibodies against SARS-CoV-2 reduces the risk of reinfection, efforts to protect HCW with risk factors for being seronegative may be needed in future COVID-19 surges. IMPORTANCE Most individuals seroconvert after infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but negative serology is observed in 1 to 9%. We found that asymptomatic or mild infection as well as a BMI above 30 were associated with being seronegative. Since the presence of antibodies against SARS-CoV-2 reduces the risk of reinfection, efforts to protect HCW with risk factors for being seronegative may be needed in future COVID-19 surges.
Keywords: SARS-CoV-2; asymptomatic infections; body mass index; health care workers; risk factor; seroconversion.
Figures
References
-
- European Centre for Disease Prevention and Control. 2021. COVID-19 situation update worldwide, as of week 23, 2021. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases. Accessed 21 June 2021.
-
- Kevadiya BD, Machhi J, Herskovitz J, Oleynikov MD, Blomberg WR, Bajwa N, Soni D, Das S, Hasan M, Patel M, Senan AM, Gorantla S, McMillan J, Edagwa B, Eisenberg R, Gurumurthy CB, Reid SPM, Punyadeera C, Chang L, Gendelman HE. 2021. Diagnostics for SARS-CoV-2 infections. Nat Mater 20:593–605. doi: 10.1038/s41563-020-00906-z. - DOI - PMC - PubMed
-
- L’Huillier AG, Meyer B, Andrey DO, Arm-Vernez I, Baggio S, Didierlaurent A, Eberhardt CS, Eckerle I, Grasset-Salomon C, Huttner A, Posfay-Barbe KM, Royo IS, Pralong JA, Vuilleumier N, Yerly S, Siegrist C-A, Kaiser L. 2021. Antibody persistence in the first 6 months following SARS-CoV-2 infection among hospital workers: a prospective longitudinal study. Clin Microbiol Infect 27:784.e1. doi: 10.1016/j.cmi.2021.01.005. - DOI - PMC - PubMed
-
- Gudbjartsson DF, Norddahl GL, Melsted P, Gunnarsdottir K, Holm H, Eythorsson E, Arnthorsson AO, Helgason D, Bjarnadottir K, Ingvarsson RF, Thorsteinsdottir B, Kristjansdottir S, Birgisdottir K, Kristinsdottir AM, Sigurdsson MI, Arnadottir GA, Ivarsdottir EV, Andresdottir M, Jonsson F, Agustsdottir AB, Berglund J, Eiriksdottir B, Fridriksdottir R, Gardarsdottir EE, Gottfredsson M, Gretarsdottir OS, Gudmundsdottir S, Gudmundsson KR, Gunnarsdottir TR, Gylfason A, Helgason A, Jensson BO, Jonasdottir A, Jonsson H, Kristjansson T, Kristinsson KG, Magnusdottir DN, Magnusson OT, Olafsdottir LB, Rognvaldsson S, Le Roux L, Sigmundsdottir G, Sigurdsson A, Sveinbjornsson G, Sveinsdottir KE, Sveinsdottir M, Thorarensen EA, Thorbjornsson B, Thordardottir M, Saemundsdottir J, et al. 2020. Humoral immune response to SARS-CoV-2 in Iceland. N Engl J Med 383:1724–1734. doi: 10.1056/NEJMoa2026116. - DOI - PMC - PubMed
-
- Lumley SF, O’Donnell D, Stoesser NE, Matthews PC, Howarth A, Hatch SB, Marsden BD, Cox S, James T, Warren F, Peck LJ, Ritter TG, de Toledo Z, Warren L, Axten D, Cornall RJ, Jones EY, Stuart DI, Screaton G, Ebner D, Hoosdally S, Chand M, Crook DW, O'Donnell A-M, Conlon CP, Pouwels KB, Walker AS, Peto TEA, Hopkins S, Walker TM, Jeffery K, Eyre DW, Oxford University Hospitals Staff Testing Group. 2021. Antibody status and incidence of SARS-CoV-2 infection in health care workers. N Engl J Med 384:533–540. doi: 10.1056/NEJMoa2034545. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
