

COVID-19-Associated Pulmonary Aspergillosis, Fungemia, and Pneumocystosis in the Intensive Care Unit: a Retrospective Multicenter Observational Cohort during the First French Pandemic Wave
- PMID: 34668768
- PMCID: PMC8528108
- DOI: 10.1128/Spectrum.01138-21
COVID-19-Associated Pulmonary Aspergillosis, Fungemia, and Pneumocystosis in the Intensive Care Unit: a Retrospective Multicenter Observational Cohort during the First French Pandemic Wave
Abstract
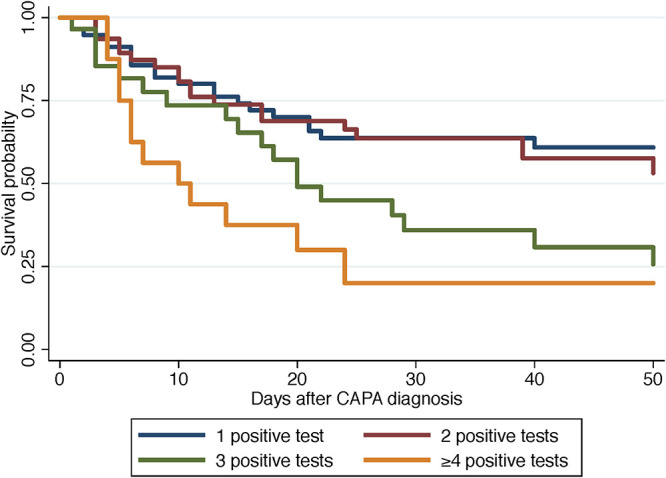
The aim of this study was to evaluate diagnostic means, host factors, delay of occurrence, and outcome of patients with COVID-19 pneumonia and fungal coinfections in the intensive care unit (ICU). From 1 February to 31 May 2020, we anonymously recorded COVID-19-associated pulmonary aspergillosis (CAPA), fungemia (CA-fungemia), and pneumocystosis (CA-PCP) from 36 centers, including results on fungal biomarkers in respiratory specimens and serum. We collected data from 154 episodes of CAPA, 81 of CA-fungemia, 17 of CA-PCP, and 5 of other mold infections from 244 patients (male/female [M/F] ratio = 3.5; mean age, 64.7 ± 10.8 years). CA-PCP occurred first after ICU admission (median, 1 day; interquartile range [IQR], 0 to 3 days), followed by CAPA (9 days; IQR, 5 to 13 days), and then CA-fungemia (16 days; IQR, 12 to 23 days) (P < 10-4). For CAPA, the presence of several mycological criteria was associated with death (P < 10-4). Serum galactomannan was rarely positive (<20%). The mortality rates were 76.7% (23/30) in patients with host factors for invasive fungal disease, 45.2% (14/31) in those with a preexisting pulmonary condition, and 36.6% (34/93) in the remaining patients (P = 0.001). Antimold treatment did not alter prognosis (P = 0.370). Candida albicans was responsible for 59.3% of CA-fungemias, with a global mortality of 45.7%. For CA-PCP, 58.8% of the episodes occurred in patients with known host factors of PCP, and the mortality rate was 29.5%. CAPA may be in part hospital acquired and could benefit from antifungal prescription at the first positive biomarker result. CA-fungemia appeared linked to ICU stay without COVID-19 specificity, while CA-PCP may not really be a concern in the ICU. Improved diagnostic strategy for fungal markers in ICU patients with COVID-19 should support these hypotheses. IMPORTANCE To diagnose fungal coinfections in patients with COVID-19 in the intensive care unit, it is necessary to implement the correct treatment and to prevent them if possible. For COVID-19-associated pulmonary aspergillosis (CAPA), respiratory specimens remain the best approach since serum biomarkers are rarely positive. Timing of occurrence suggests that CAPA could be hospital acquired. The associated mortality varies from 36.6% to 76.7% when no host factors or host factors of invasive fungal diseases are present, respectively. Fungemias occurred after 2 weeks in ICUs and are associated with a mortality rate of 45.7%. Candida albicans is the first yeast species recovered, with no specificity linked to COVID-19. Pneumocystosis was mainly found in patients with known immunodepression. The diagnosis occurred at the entry in ICUs and not afterwards, suggesting that if Pneumocystis jirovecii plays a role, it is upstream of the hospitalization in the ICU.
Keywords: Aspergillus; COVID-19; France; aspergillosis; critical care; fungemia; pneumocystosis.
Figures


References
-
- Verweij PE, Rijnders BJA, Brüggemann RJM, Azoulay E, Bassetti M, Blot S, Calandra T, Clancy CJ, Cornely OA, Chiller T, Depuydt P, Giacobbe DR, Janssen NAF, Kullberg B-J, Lagrou K, Lass-Florl C, Lewis RE, Liu PW-L, Lortholary O, Maertens J, Martin-Loeches I, Nguyen MH, Patterson TF, Rogers TR, Schouten JA, Spriet I, Vanderbeke L, Wauters J, van de Veerdonk FL. 2020. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med 46:1524–1535. doi: 10.1007/s00134-020-06091-6. - DOI - PMC - PubMed
-
- Schauwvlieghe AFAD, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, Van Tienen C, Lagrou K, Verweij PE, van de Veerdonk FL, Gommers D, Spronk P, Bergmans DCJJ, Hoedemaekers A, Andrinopoulou E-R, van den Berg CHSB, Juffermans NP, Hodiamont CJ, Vonk AG, Depuydt P, Boelens J, Wauters J, Dutch-Belgian Mycosis Study Group. 2018. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med 6:782–792. doi: 10.1016/S2213-2600(18)30274-1. - DOI - PubMed
-
- White PL, Dhillon R, Cordey A, Hughes H, Faggian F, Soni S, Pandey M, Whitaker H, May A, Morgan M, Wise MP, Healy B, Blyth I, Price JS, Vale L, Posso R, Kronda J, Blackwood A, Rafferty H, Moffitt A, Tsitsopoulou A, Gaur S, Holmes T, Backx M. 2020. A national strategy to diagnose COVID-19 associated invasive fungal disease in the ICU. Clin Infect Dis 56:e01122. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
