

Surgical Treatment of Postinfarction Ventricular Septal Rupture
- PMID: 34668946
- PMCID: PMC8529403
- DOI: 10.1001/jamanetworkopen.2021.28309
Surgical Treatment of Postinfarction Ventricular Septal Rupture
Abstract
Importance: Ventricular septal rupture (VSR) is a rare but life-threatening mechanical complication of acute myocardial infarction associated with high mortality despite prompt treatment. Surgery represents the standard of care; however, only small single-center series or national registries are usually available in literature, whereas international multicenter investigations have been poorly carried out, therefore limiting the evidence on this topic.
Objectives: To assess the clinical characteristics and early outcomes for patients who received surgery for postinfarction VSR and to identify factors independently associated with mortality.
Design, setting, and participants: The Mechanical Complications of Acute Myocardial Infarction: an International Multicenter Cohort (CAUTION) Study is a retrospective multicenter international cohort study that includes patients who were treated surgically for mechanical complications of acute myocardial infarction. The study was conducted from January 2001 to December 2019 at 26 different centers worldwide among 475 consecutive patients who underwent surgery for postinfarction VSR.
Exposures: Surgical treatment of postinfarction VSR, independent of the technique, alone or combined with other procedures (eg, coronary artery bypass grafting).
Main outcomes and measures: The primary outcome was early mortality; secondary outcomes were postoperative complications.
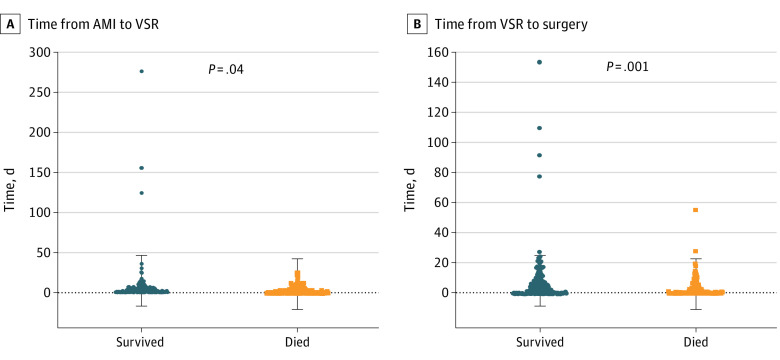
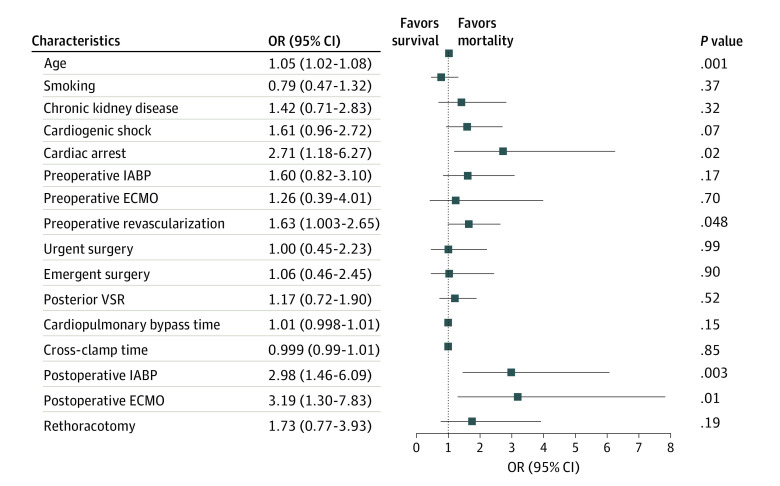
Results: Of the 475 patients included in the study, 290 (61.1%) were men, with a mean (SD) age of 68.5 (10.1) years. Cardiogenic shock was present in 213 patients (44.8%). Emergent or salvage surgery was performed in 212 cases (44.6%). The early mortality rate was 40.4% (192 patients), and it did not improve during the nearly 20 years considered for the study (median [IQR] yearly mortality, 41.7% [32.6%-50.0%]). Low cardiac output syndrome and multiorgan failure were the most common causes of death (low cardiac output syndrome, 70 [36.5%]; multiorgan failure, 53 [27.6%]). Recurrent VSR occurred in 59 participants (12.4%) but was not associated with mortality. Cardiogenic shock (survived: 95 [33.6%]; died, 118 [61.5%]; P < .001) and early surgery (time to surgery ≥7 days, survived: 105 [57.4%]; died, 47 [35.1%]; P < .001) were associated with lower survival. At multivariate analysis, older age (odds ratio [OR], 1.05; 95% CI, 1.02-1.08; P = .001), preoperative cardiac arrest (OR, 2.71; 95% CI, 1.18-6.27; P = .02) and percutaneous revascularization (OR, 1.63; 95% CI, 1.003-2.65; P = .048), and postoperative need for intra-aortic balloon pump (OR, 2.98; 95% CI, 1.46-6.09; P = .003) and extracorporeal membrane oxygenation (OR, 3.19; 95% CI, 1.30-7.38; P = .01) were independently associated with mortality.
Conclusions and relevance: In this study, surgical repair of postinfarction VSR was associated with a high risk of early mortality; this risk has remained unchanged during the last 2 decades. Delayed surgery seemed associated with better survival. Age, preoperative cardiac arrest and percutaneous revascularization, and postoperative need for intra-aortic balloon pump and extracorporeal membrane oxygenation were independently associated with early mortality. Further prospective studies addressing preoperative and perioperative patient management are warranted to hopefully improve the currently suboptimal outcome.
Conflict of interest statement
Figures
References
-
- Arnaoutakis GJ, Zhao Y, George TJ, Sciortino CM, McCarthy PM, Conte JV. Surgical repair of ventricular septal defect after myocardial infarction: outcomes from the Society of Thoracic Surgeons National Database. Ann Thorac Surg. 2012;94(2):436-443. doi: 10.1016/j.athoracsur.2012.04.020 - DOI - PMC - PubMed
-
- Crenshaw BS, Granger CB, Birnbaum Y, et al. ; GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators . Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. Circulation. 2000;101(1):27-32. doi: 10.1161/01.CIR.101.1.27 - DOI - PubMed
