

Strategies for Antibiotic Administration for Bowel Preparation Among Patients Undergoing Elective Colorectal Surgery: A Network Meta-analysis
- PMID: 34668964
- PMCID: PMC8529526
- DOI: 10.1001/jamasurg.2021.5251
Strategies for Antibiotic Administration for Bowel Preparation Among Patients Undergoing Elective Colorectal Surgery: A Network Meta-analysis
Abstract
Importance: There are discrepancies in guidelines on preparation for colorectal surgery. While intravenous (IV) antibiotics are usually administered, the use of mechanical bowel preparation (MBP), enemas, and/or oral antibiotics (OA) is controversial.
Objective: To summarize all data from randomized clinical trials (RCTs) that met selection criteria using network meta-analysis (NMA) to determine the ranking of different bowel preparation treatment strategies for their associations with postoperative outcomes.
Data sources: Data sources included MEDLINE, Embase, Cochrane, and Scopus databases with no language constraints, including abstracts and articles published prior to 2021.
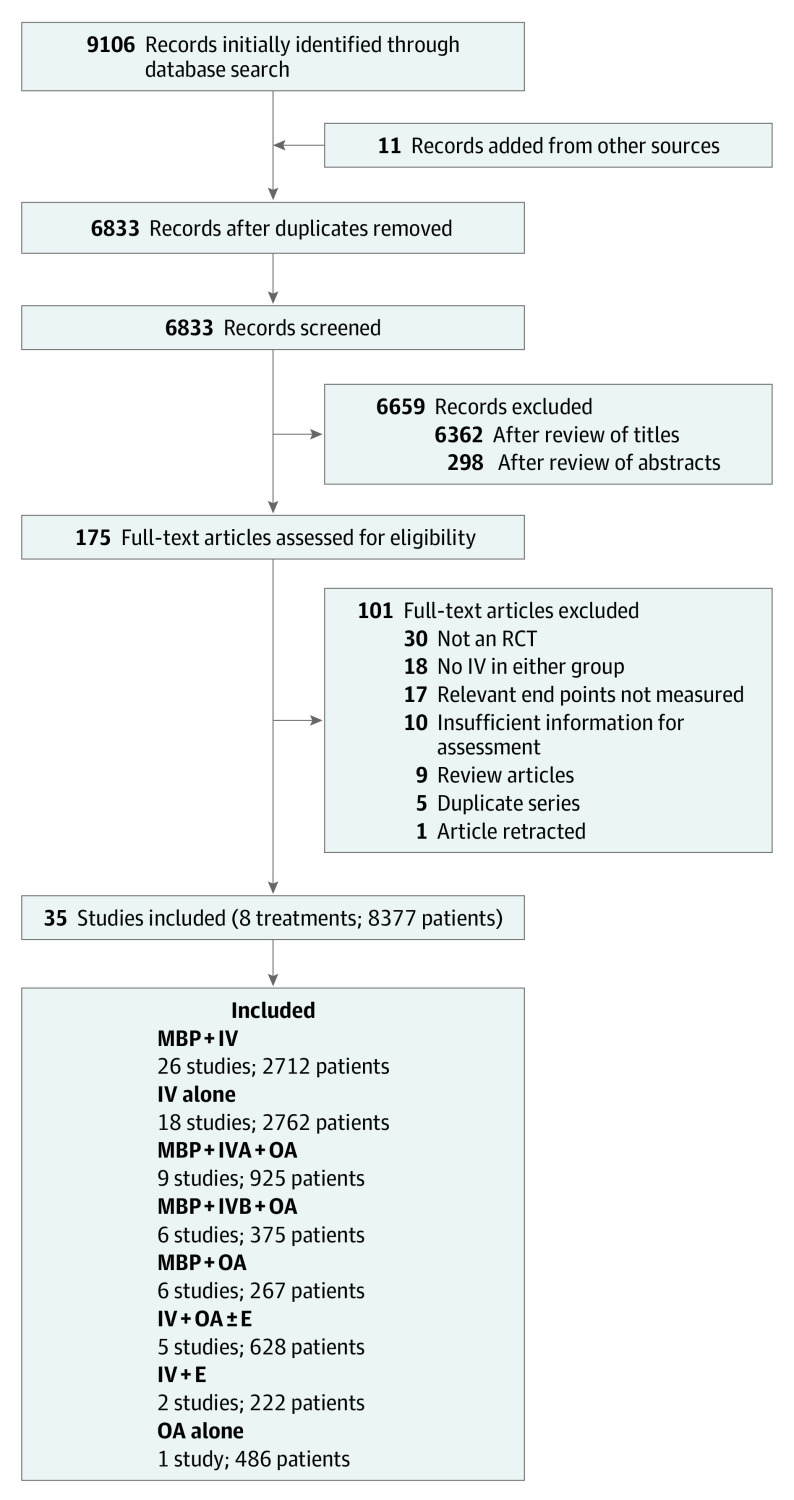
Study selection: Randomized studies of adults undergoing elective colorectal surgery with appropriate aerobic and anaerobic antibiotic cover that reported on incisional surgical site infection (SSI) or anastomotic leak were selected for inclusion in the analysis. These were selected by multiple reviewers and adjudicated by a separate lead investigator. A total of 167 of 6833 screened studies met initial selection criteria.
Data extraction and synthesis: NMA was performed according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines. Data were extracted by multiple independent observers and pooled in a random-effects model.
Main outcomes and measures: Primary outcomes were incisional SSI and anastomotic leak. Secondary outcomes included other infections, mortality, ileus, and adverse effects of preparation.
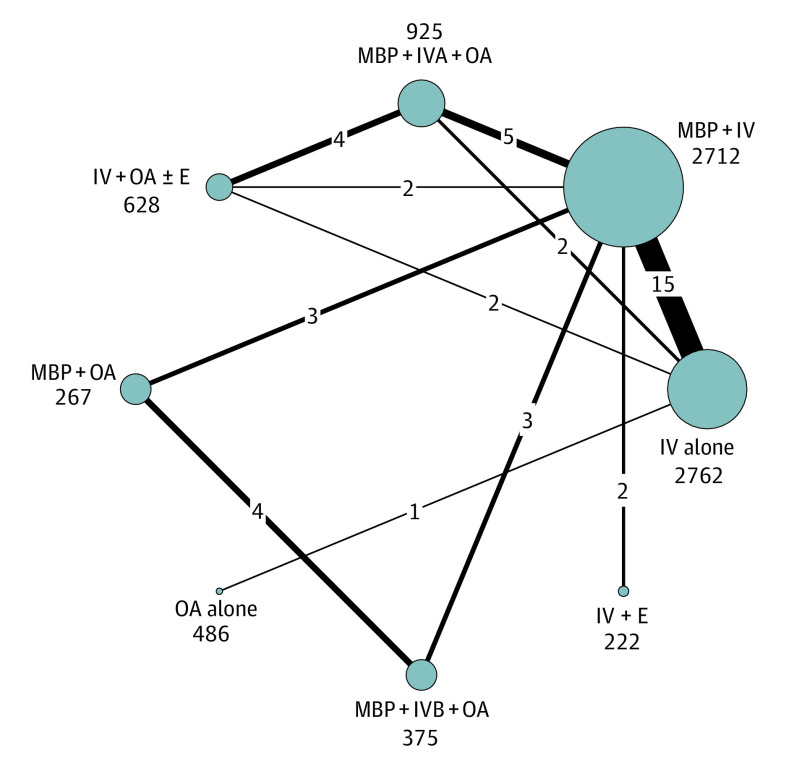
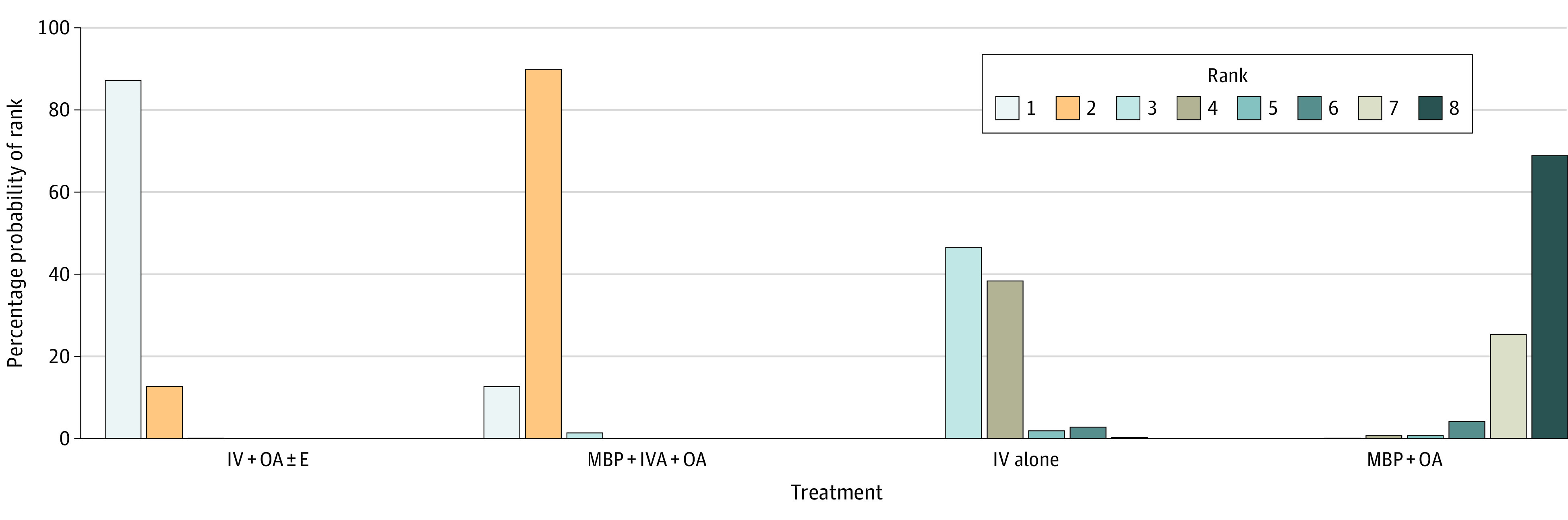
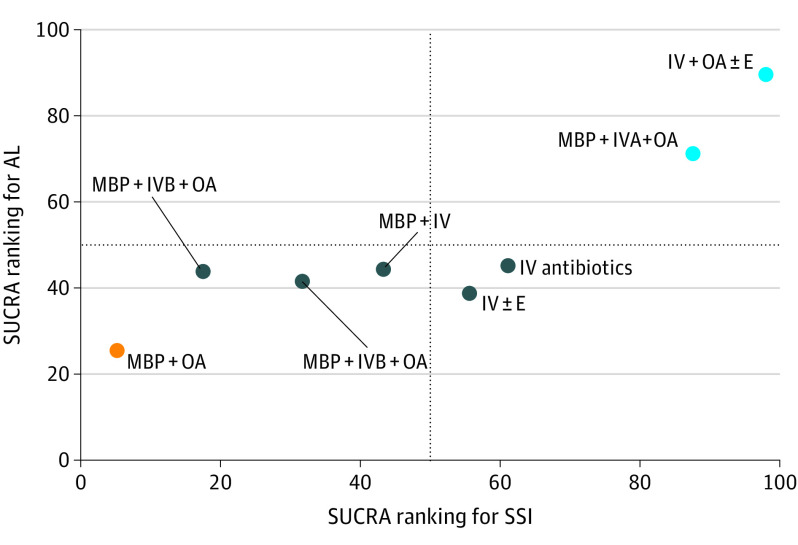
Results: A total of 35 RCTs that included 8377 patients were identified. Treatments compared IV antibiotics (2762 patients [33%]), IV antibiotics with enema (222 patients [3%]), IV antibiotics with OA with or without enema (628 patients [7%]), MBP with IV antibiotics (2712 patients [32%]), MBP with IV antibiotics with OA (with good IV antibiotic cover in 925 patients [11%] and with good overall antibiotic cover in 375 patients [4%]), MBP with OA (267 patients [3%]), and OA (486 patients [6%]). The likelihood of incisional SSI was significantly lower for those receiving IV antibiotics with OA with or without enema (rank 1) and MBP with adequate IV antibiotics with OA (rank 2) compared with all other treatment options. The addition of OA to IV antibiotics, both with and without MBP, was associated with a reduction in incisional SSI by greater than 50%. There were minimal differences between treatments in anastomotic leak and in any of the secondary outcomes.
Conclusions and relevance: This NMA demonstrated that the addition of OA to IV antibiotics were associated with a reduction in incisional SSI by greater than 50%. The results support the addition of OA to IV antibiotics to reduce incisional SSI among patients undergoing elective colorectal surgery.
Conflict of interest statement
Figures
Comment on
-
Bowel Preparation for Colorectal Surgery: Have All Questions Been Answered?JAMA Surg. 2022 Jan 1;157(1):41-42. doi: 10.1001/jamasurg.2021.5273. JAMA Surg. 2022. PMID: 34668973 No abstract available.
References
-
- Gordon P, Nivatvongs S. Principles and Practice of Surgery for the Colon, Rectum, and Anus. 2nd ed. Quality Medical Publishing. 1999.
-
- Clarke JS, Condon RE, Bartlett JG, Gorbach SL, Nichols RL, Ochi S. Preoperative oral antibiotics reduce septic complications of colon operations: results of prospective, randomized, double-blind clinical study. Ann Surg. 1977;186(3):251-259. doi: 10.1097/00000658-197709000-00003 - DOI - PMC - PubMed
-
- Keighley MR., Arabi Y, Alexander-Williams J. Which is the best route of antibiotic prophylaxis in elective colorectal surgery: oral or parenteral? Gut. 1979;20:A453.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
