

Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): an updated European Academy of Paediatric Dentistry policy document
- PMID: 34669177
- PMCID: PMC8926988
- DOI: 10.1007/s40368-021-00668-5
Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): an updated European Academy of Paediatric Dentistry policy document
Abstract
Aim: To update the existing European Academy of Paediatric Dentistry (EAPD) 2010 policy document on the 'Best Clinical Practice guidance for clinicians dealing with children presenting with Molar-Incisor-Hypomineralisation (MIH).'
Methods: Experts, assigned the EAPD, worked on two different topics: (A) Aetiological factors involved in MIH, and (B) Treatment options for the clinical management of MIH. The group prepared two detailed systematic reviews of the existing literature relevant to the topics and following a consensus process produced the updated EAPD policy document on the 'Best Clinical Practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH).' The GRADE system was used to assess the quality of evidence regarding aetiology and treatment which was judged as HIGH, MODERATE, LOW or VERY LOW, while the GRADE criteria were used to indicate the strength of recommendation regarding treatment options as STRONG or WEAK/CONDITIONAL.
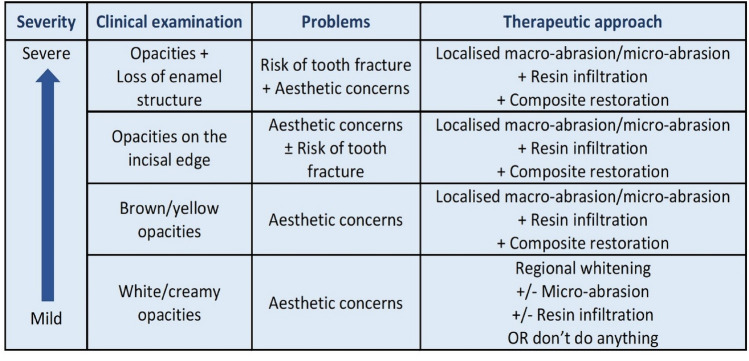
Results: (A) Regarding aetiology, it is confirmed that MIH has a multifactorial aetiology with the duration, strength and timing of occurrence of the aetiological factors being responsible for the variable clinical characteristics of the defect. Perinatal hypoxia, prematurity and other hypoxia related perinatal problems, including caesarean section, appear to increase the risk of having MIH, while certain infant and childhood illnesses are also linked with MIH. In addition, genetic predisposition and the role of epigenetic influences are becoming clearer following twin studies and genome and single-nucleotide polymorphisms analyses in patients and families. Missing genetic information might be the final key to truly understand MIH aetiology. (B) Regarding treatment options, composite restorations, preformed metal crowns and laboratory indirect restorations provide high success rates for the posterior teeth in appropriate cases, while scheduled extractions provide an established alternative option in severe cases. There is great need for further clinical and laboratory studies evaluating new materials and non-invasive/micro-invasive techniques for anterior teeth, especially when aesthetic and oral health related quality of life (OHRQoL) issues are concerned.
Conclusions: MIH has been studied more extensively in the last decade. Its aetiology follows the multifactorial model, involving systemic medical and genetic factors. Further focused laboratory research and prospective clinical studies are needed to elucidate any additional factors and refine the model. Successful preventive and treatment options have been studied and established. The appropriate choice depends on the severity of the defects and the age of the patient. EAPD encourages the use of all available treatment options, whilst in severe cases, scheduled extractions should be considered.
Keywords: Aetiology; Clinical practice; EAPD; Guidelines; MIH; Molar incisor hypomineralisation; Policy document; Treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
20 years of research into the aetiology of molar-incisor hypomineralization.Eur Arch Paediatr Dent. 2023 Apr;24(2):273-274. doi: 10.1007/s40368-022-00774-y. Epub 2023 Jan 24. Eur Arch Paediatr Dent. 2023. PMID: 36692667 No abstract available.
-
MIH should be a core component of every dental curriculum.Eur Arch Paediatr Dent. 2023 Jun;24(3):427-428. doi: 10.1007/s40368-023-00810-5. Epub 2023 Jun 12. Eur Arch Paediatr Dent. 2023. PMID: 37306867 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
