

Functional Effects of Cardiomyocyte Injury in COVID-19
- PMID: 34669512
- PMCID: PMC8791272
- DOI: 10.1128/JVI.01063-21
Functional Effects of Cardiomyocyte Injury in COVID-19
Abstract
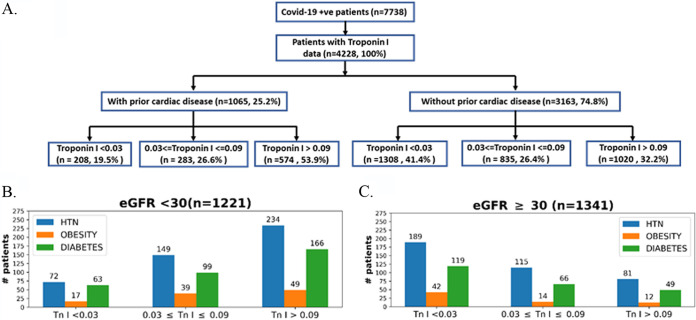
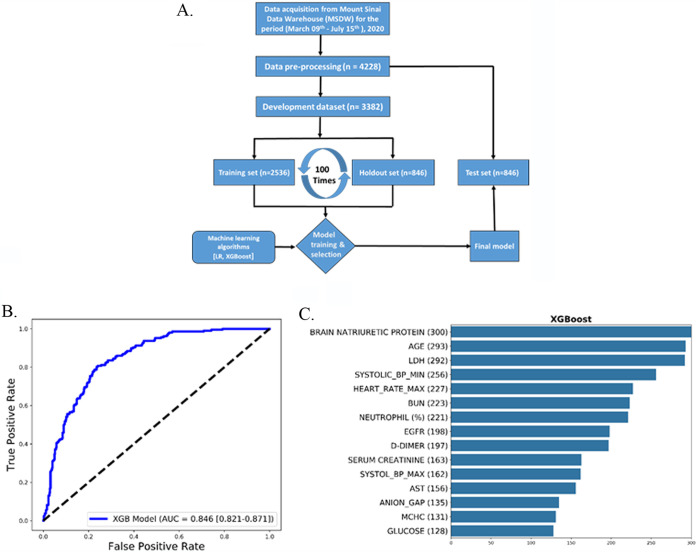
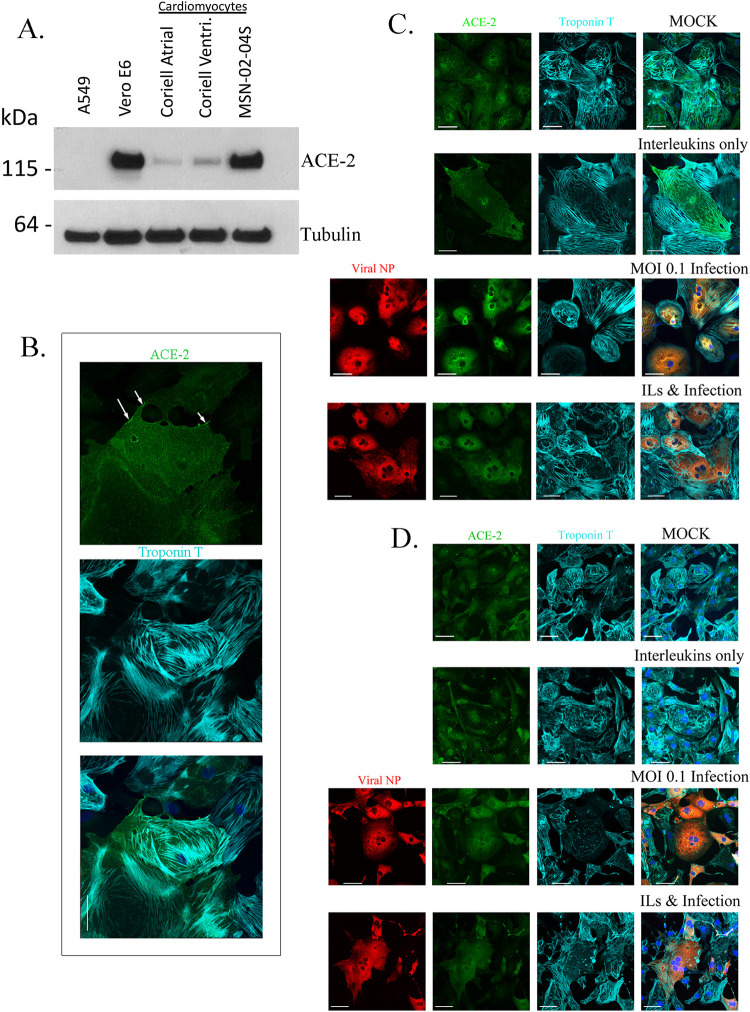
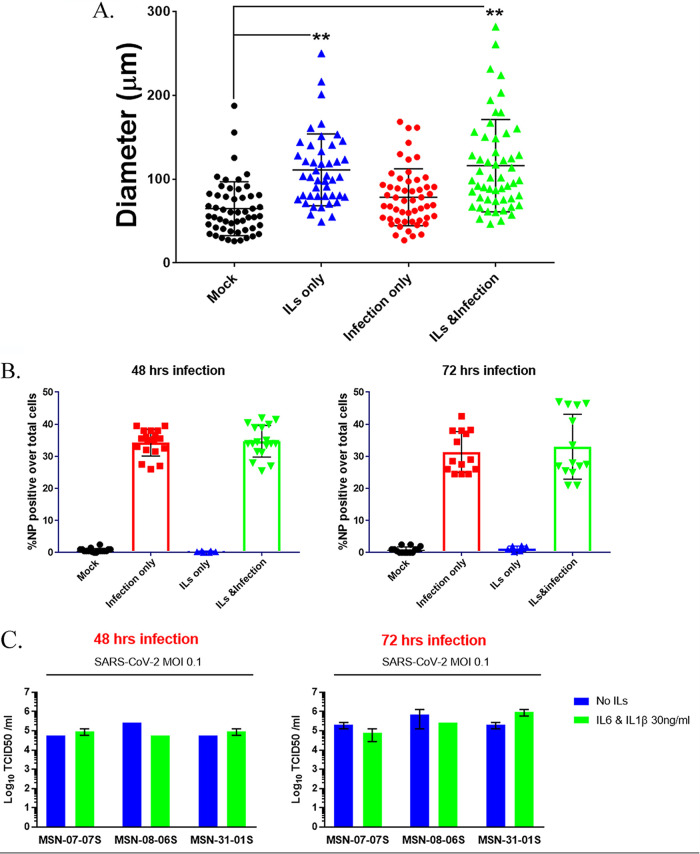
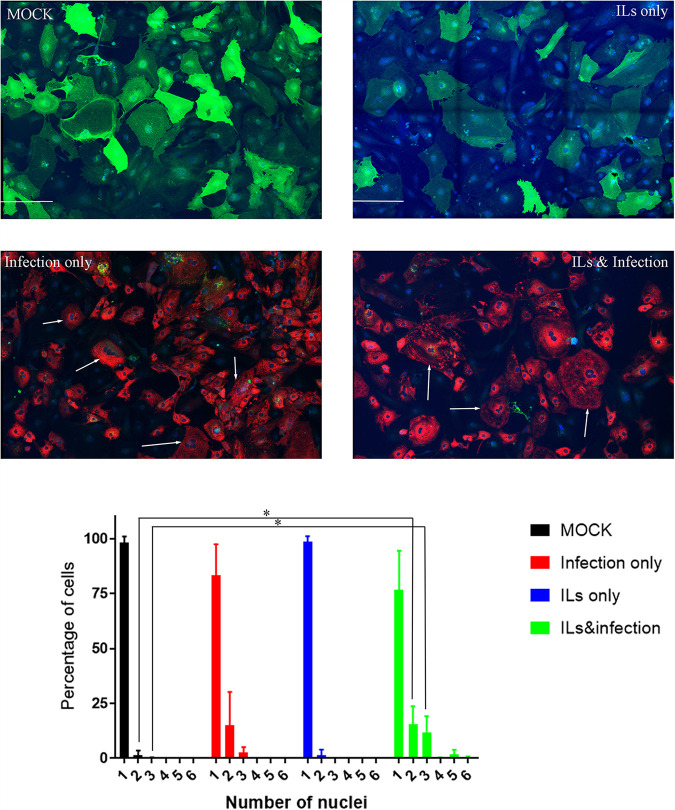
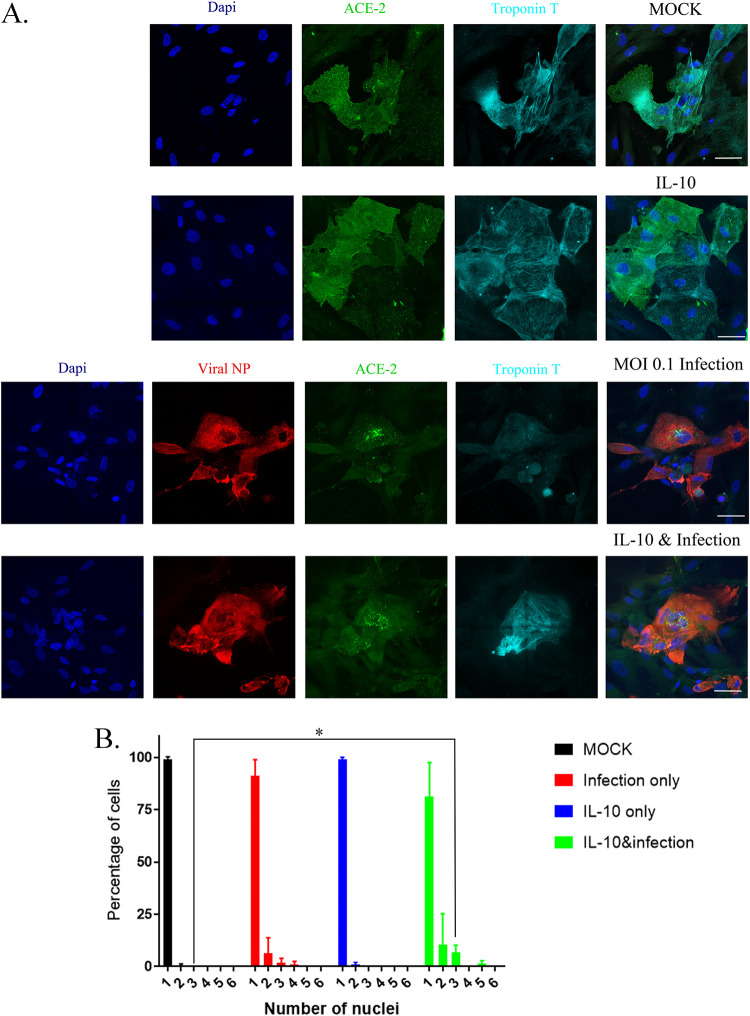
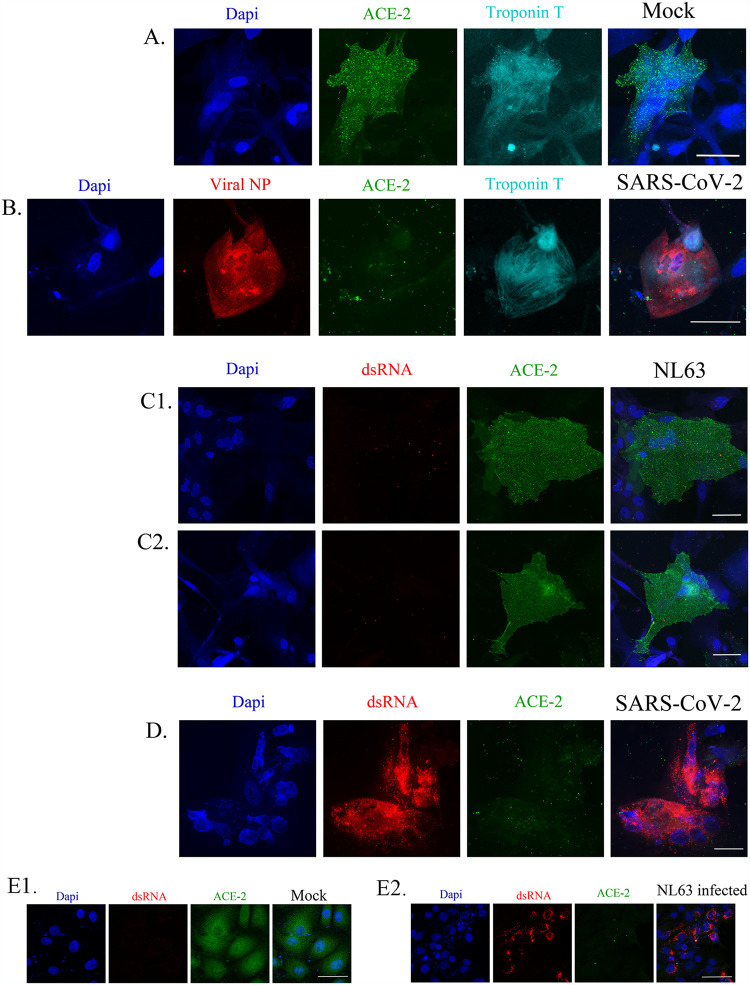
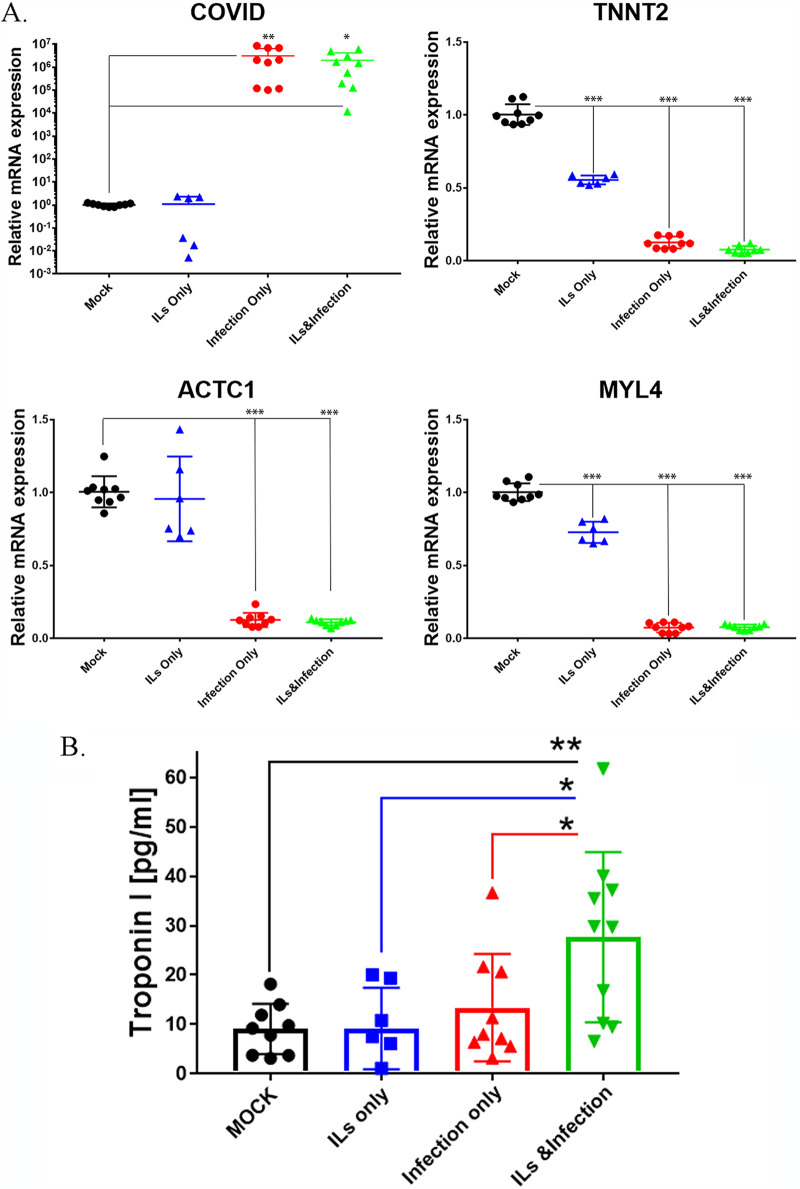
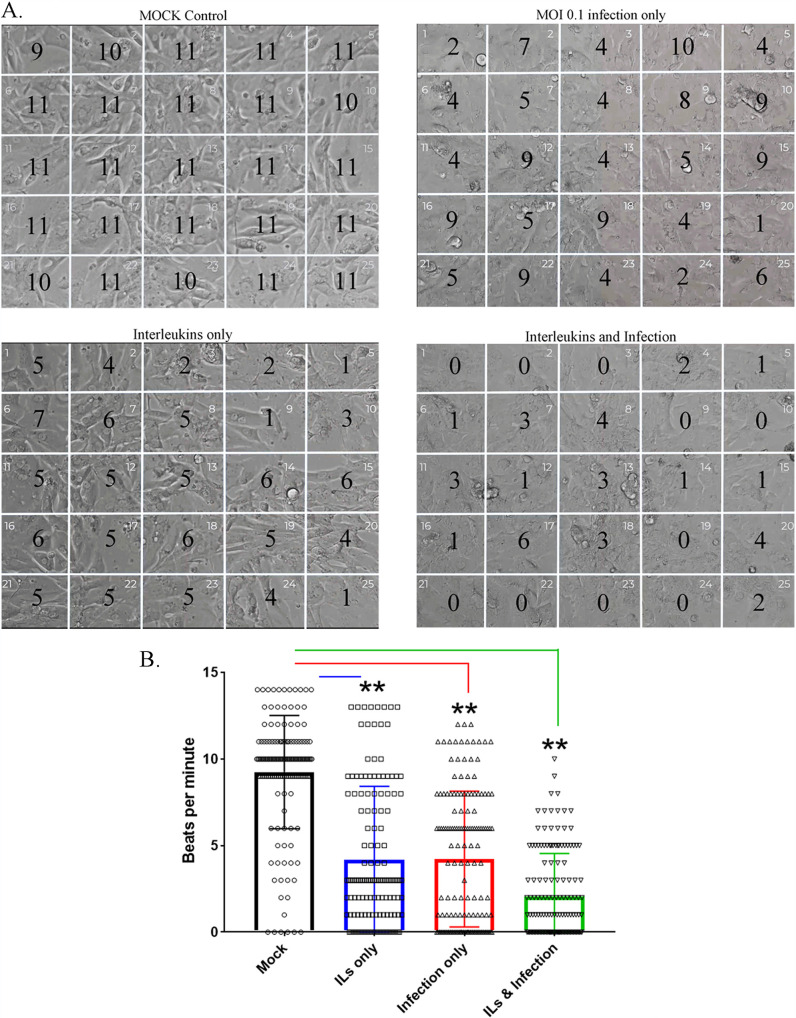
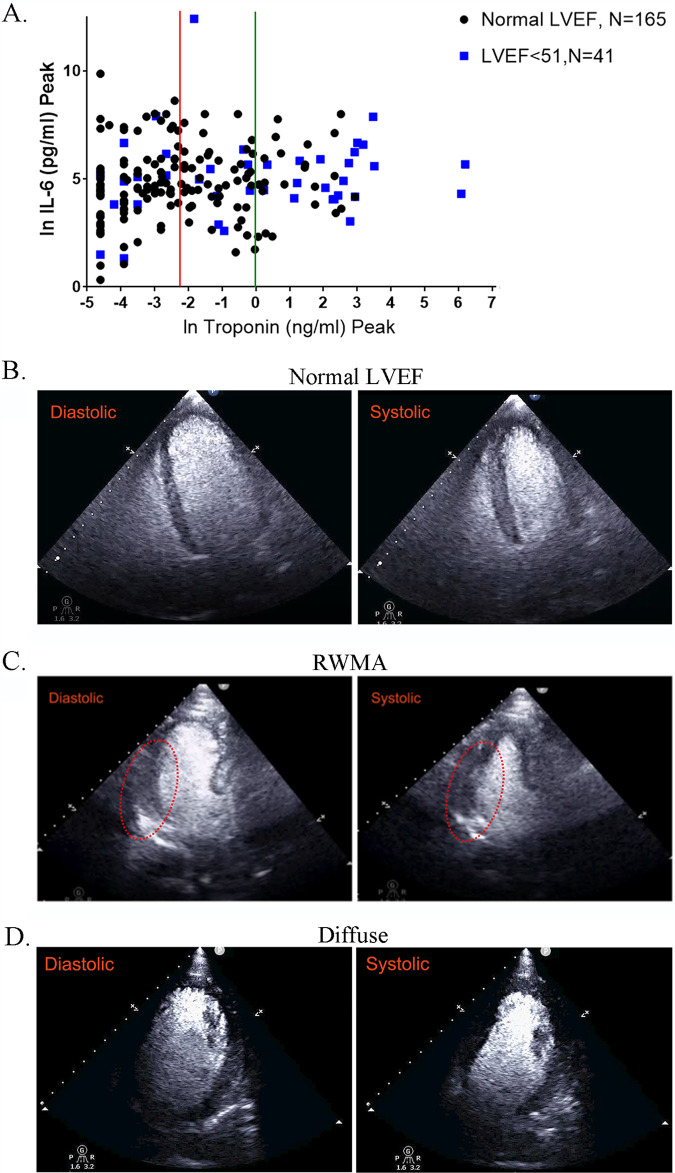
COVID-19 affects multiple organs. Clinical data from the Mount Sinai Health System show that substantial numbers of COVID-19 patients without prior heart disease develop cardiac dysfunction. How COVID-19 patients develop cardiac disease is not known. We integrated cell biological and physiological analyses of human cardiomyocytes differentiated from human induced pluripotent stem cells (hiPSCs) infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the presence of interleukins (ILs) with clinical findings related to laboratory values in COVID-19 patients to identify plausible mechanisms of cardiac disease in COVID-19 patients. We infected hiPSC-derived cardiomyocytes from healthy human subjects with SARS-CoV-2 in the absence and presence of IL-6 and IL-1β. Infection resulted in increased numbers of multinucleated cells. Interleukin treatment and infection resulted in disorganization of myofibrils, extracellular release of troponin I, and reduced and erratic beating. Infection resulted in decreased expression of mRNA encoding key proteins of the cardiomyocyte contractile apparatus. Although interleukins did not increase the extent of infection, they increased the contractile dysfunction associated with viral infection of cardiomyocytes, resulting in cessation of beating. Clinical data from hospitalized patients from the Mount Sinai Health System show that a significant portion of COVID-19 patients without history of heart disease have elevated troponin and interleukin levels. A substantial subset of these patients showed reduced left ventricular function by echocardiography. Our laboratory observations, combined with the clinical data, indicate that direct effects on cardiomyocytes by interleukins and SARS-CoV-2 infection might underlie heart disease in COVID-19 patients. IMPORTANCE SARS-CoV-2 infects multiple organs, including the heart. Analyses of hospitalized patients show that a substantial number without prior indication of heart disease or comorbidities show significant injury to heart tissue, assessed by increased levels of troponin in blood. We studied the cell biological and physiological effects of virus infection of healthy human iPSC-derived cardiomyocytes in culture. Virus infection with interleukins disorganizes myofibrils, increases cell size and the numbers of multinucleated cells, and suppresses the expression of proteins of the contractile apparatus. Viral infection of cardiomyocytes in culture triggers release of troponin similar to elevation in levels of COVID-19 patients with heart disease. Viral infection in the presence of interleukins slows down and desynchronizes the beating of cardiomyocytes in culture. The cell-level physiological changes are similar to decreases in left ventricular ejection seen in imaging of patients' hearts. These observations suggest that direct injury to heart tissue by virus can be one underlying cause of heart disease in COVID-19.
Keywords: COVID-19; IL-10; IL-1β; IL-6; NL63; SARS-CoV-2; cardiac disease; cardiomyocytes; computational biology; machine learning.
Figures
Update of
-
Physiology of cardiomyocyte injury in COVID-19.medRxiv [Preprint]. 2020 Nov 16:2020.11.10.20229294. doi: 10.1101/2020.11.10.20229294. medRxiv. 2020. Update in: J Virol. 2022 Jan 26;96(2):e0106321. doi: 10.1128/JVI.01063-21. PMID: 33200140 Free PMC article. Updated. Preprint.
References
-
- New York Times. 2020. Coronavirus world map: tracking the global outbreak. https://www.nytimes.com/interactive/2020/world/coronavirus-maps.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
