

Asthma Phenotypes and COVID-19 Risk: A Population-based Observational Study
- PMID: 34669568
- PMCID: PMC8865578
- DOI: 10.1164/rccm.202107-1704OC
Asthma Phenotypes and COVID-19 Risk: A Population-based Observational Study
Abstract
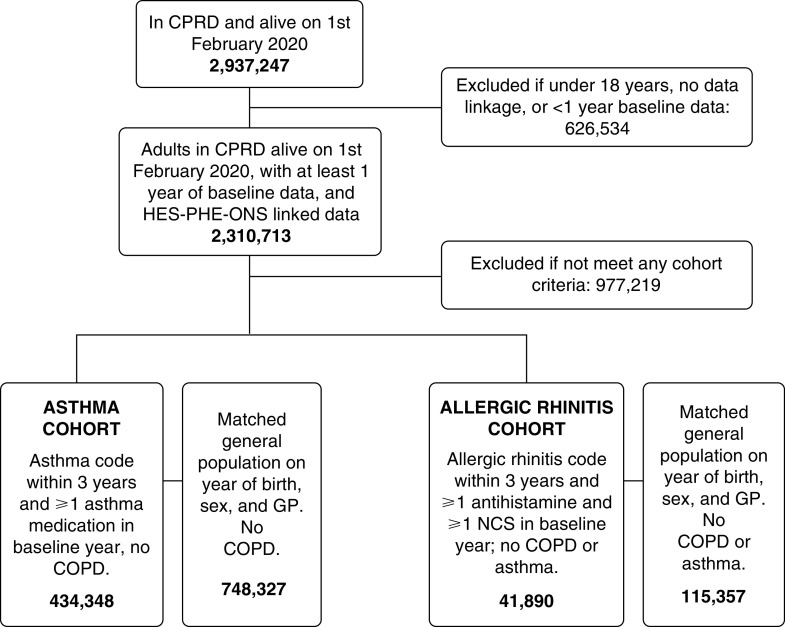
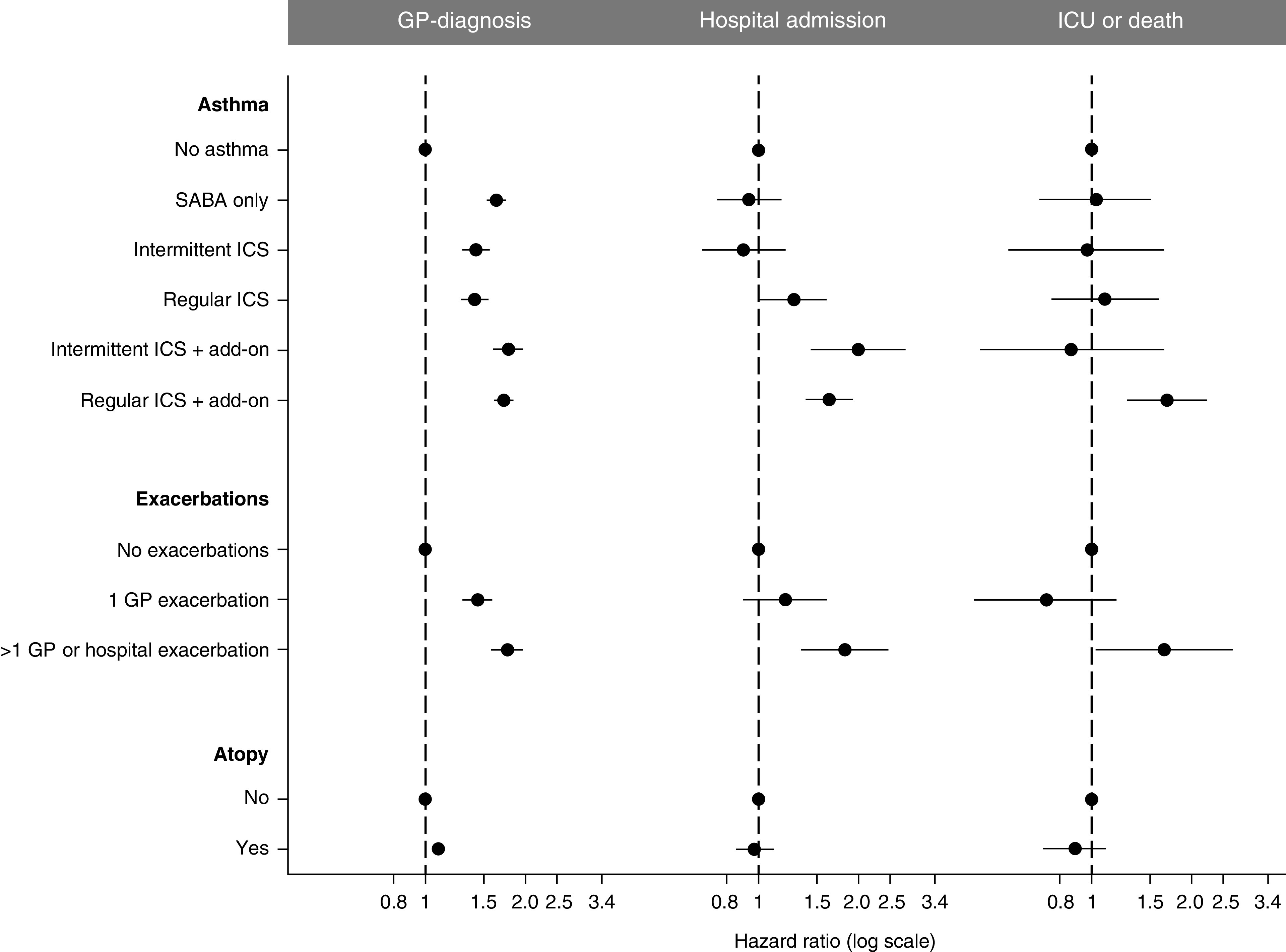
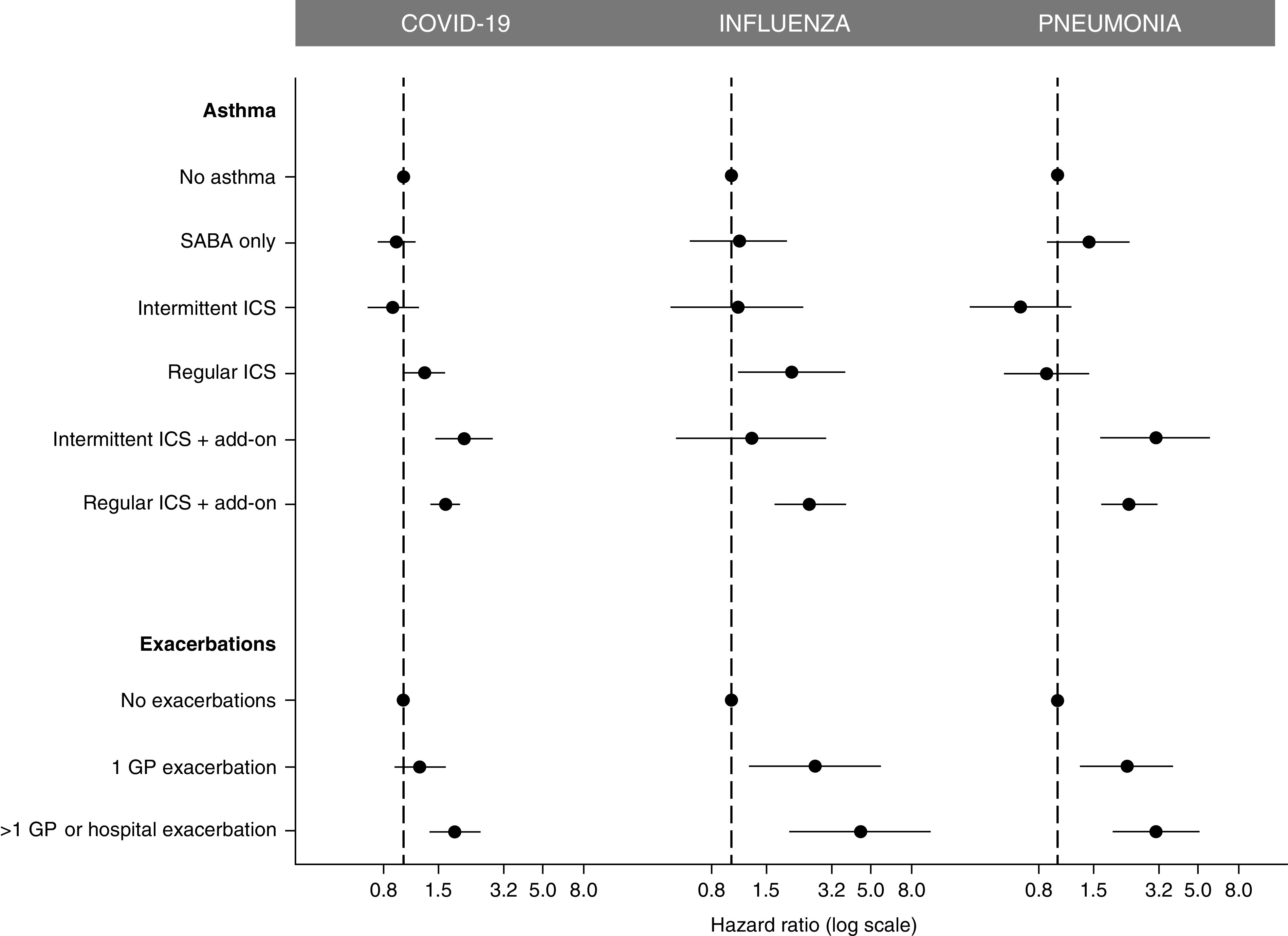
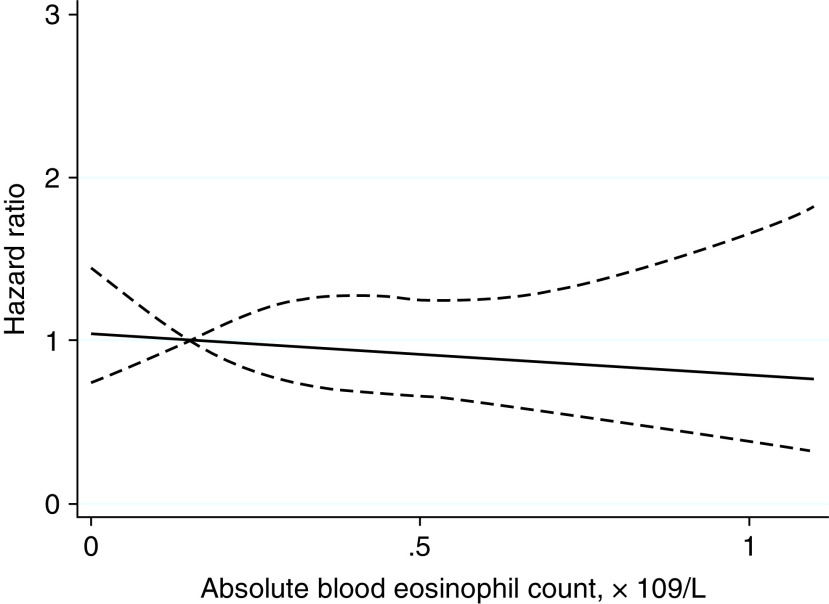
Rationale: Studies have suggested some patients with asthma are at risk of severe coronavirus disease (COVID-19), but they have had limited data on asthma phenotype and have not considered if risks are specific to COVID-19. Objectives: To determine the effect of asthma phenotype on three levels of COVID-19 outcomes. Compare hospitalization rates with influenza and pneumonia. Methods: Electronic medical records were used to identify patients with asthma and match them to the general population. Patient-level data were linked to Public Health England severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) test data, hospital, and mortality data. Asthma was phenotyped by medication, exacerbation history, and type 2 inflammation. The risk of each outcome, adjusted for major risk factors, was measured using Cox regression. Measurements and Main Results: A total of 434,348 patients with asthma and 748,327 matched patients were included. All patients with asthma had a significantly increased risk of a General Practice diagnosis of COVID-19. Asthma with regular inhaled corticosteroid (ICS) use (hazard ratio [HR], 1.27; 95% confidence interval [CI], 1.01-1.61), intermittent ICS plus add-on asthma medication use (HR, 2.00; 95% CI, 1.43-2.79), regular ICS plus add-on use (HR, 1.63; 95% CI, 1.37-1.94), or with frequent exacerbations (HR, 1.82; 95% CI, 1.34-2.47) was significantly associated with hospitalization. These phenotypes were significantly associated with influenza and pneumonia hospitalizations. Only patients with regular ICS plus add-on asthma therapy (HR, 1.70; 95% CI, 1.27-2.26) or frequent exacerbations (HR, 1.66; 95% CI, 1.03-2.68) had a significantly higher risk of ICU admission or death. Atopy and blood eosinophil count were not associated with severe COVID-19 outcomes. Conclusions: More severe asthma was associated with more severe COVID-19 outcomes, but type 2 inflammation was not. The risk of COVID-19 hospitalization appeared to be similar to the risk with influenza or pneumonia.
Keywords: COVID-19; allergic rhinitis; asthma; disease severity; influenza.
Figures
Comment in
-
Gaining Insights into Asthma-related COVID-19 Risk.Am J Respir Crit Care Med. 2022 Jan 1;205(1):1-2. doi: 10.1164/rccm.202111-2473ED. Am J Respir Crit Care Med. 2022. PMID: 34813725 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
