

WHAT FACTORS CONTRIBUTE TO DELAYED GASTRIC EMPTYING AFTER DUODENOPANCREATECTOMY WITH PILORIC PRESERVATION?
- PMID: 34669882
- PMCID: PMC8521836
- DOI: 10.1590/0102-672020210002e1592
WHAT FACTORS CONTRIBUTE TO DELAYED GASTRIC EMPTYING AFTER DUODENOPANCREATECTOMY WITH PILORIC PRESERVATION?
Abstract
Background: The delay in gastric emptying is the second most frequent complication after duodenopancreatectomy with pyloric preservation, that increases hospitalization time and hospital costs.
Aim: To identify factors that contribute to the appearance the delay in this surgical procedure.
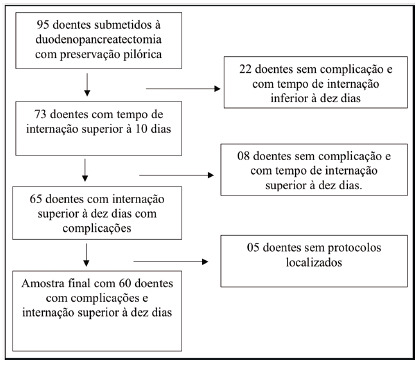
Method: Ninety-five patients were submitted to duodenopancreatectomy with pyloric preservation. After retrospective analysis of the medical records, it was observed that 60 had prolonged hospitalization due to complications. Thus, univariate and multivariate logistic regression were used to analyze predictors of delayed gastric emptying.
Results: Delay was present in 65% (n=39) and pancreatic fistula in 38.3% (n=23). Univariate analysis revealed that the presence of pancreatic complications (pancreatic fistula, p=0.01), other intracavitary complications with the appearance of abdominal collections (p=0.03) and hypoalbuminemia (p=0.06) were responsible, also confirmed by the multivariate analysis. In those who presented delay without a determined cause, it was observed that high levels of total bilirubin (p=0.01) and direct bilirubin (p=0.01) could be related to it.
Conclusion: The delay in gastric emptying in patients undergoing duodenopancreatectomy with pyloric preservation is due to intracavitary complications.
Racional:: O retardo do esvaziamento gástrico é a segunda complicação mais frequente após a realização da duodenopancreatectomia com preservação pilórica, aumentando o tempo de internação e custos hospitalares.
Objetivo:: Identificar fatores que contribuem para o aparecimento desse retardo nesse procedimento cirúrgico.
Método:: Noventa e cinco doentes foram submetidos à duodenopancreatectomia com preservação pilórica. Após análise retrospectiva dos prontuários observou-se que 60 apresentaram internação prolongada por complicações. Assim, utilizou-se a regressão logística uni e multivariada para análise de fatores preditores do retardo.
Resultados:: O retardo esteve presente em 65% (n=39) e a fístula pancreática em 38,3% (n=23). A análise univariada revelou que a presença de complicações pancreáticas (fístula pancreática, p=0,01), outras complicações intracavitárias com aparecimento de coleções abdominais (p=0,03) e hipoalbuminemia (p=0,06) foram os responsáveis, resultados estes também confirmados pela análise mutilvariada. Naqueles que apresentaram retardo sem causa determinada, observou-se que níveis elevados de bilirrubina total (p=0,01) e bilirrubina direta (p=0,01) poderiam estar relacionados a ele.
Conclusão:: O retardo do esvaziamento gástrico nos pacientes submetidos à duodenopancreatectomia com preservação pilórica é decorrente de complicações intracavitárias.
Conflict of interest statement
Figures




References
-
- Balzano G, Zerbi A, Braga M, Rocchetti S, Beneduce AA, Di Carlo V. Fast-track recovery programme after pancreaticoduodenectomy reduced delayed gastric emptying. Br J Surg. 2008;95:1387–1393. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
