

Geographic and Regional Variability in Racial and Ethnic Disparities in Stroke Thrombolysis in the United States
- PMID: 34670410
- PMCID: PMC8608741
- DOI: 10.1161/STROKEAHA.121.035220
Geographic and Regional Variability in Racial and Ethnic Disparities in Stroke Thrombolysis in the United States
Abstract
Background and purpose: Intravenous thrombolysis (IVT) after ischemic stroke is underutilized in racially/ethnically minoritized groups. We aimed to determine the regional and geographic variability in racial/ethnic IVT disparities in the United States.
Methods: Acute ischemic stroke admissions between 2012 and 2018 were identified in the National Inpatient Sample. Multivariable logistic regression was used to test the association between IVT and race/ethnicity, stratified by geographic region and controlling for demographic, clinical, and hospital characteristics.
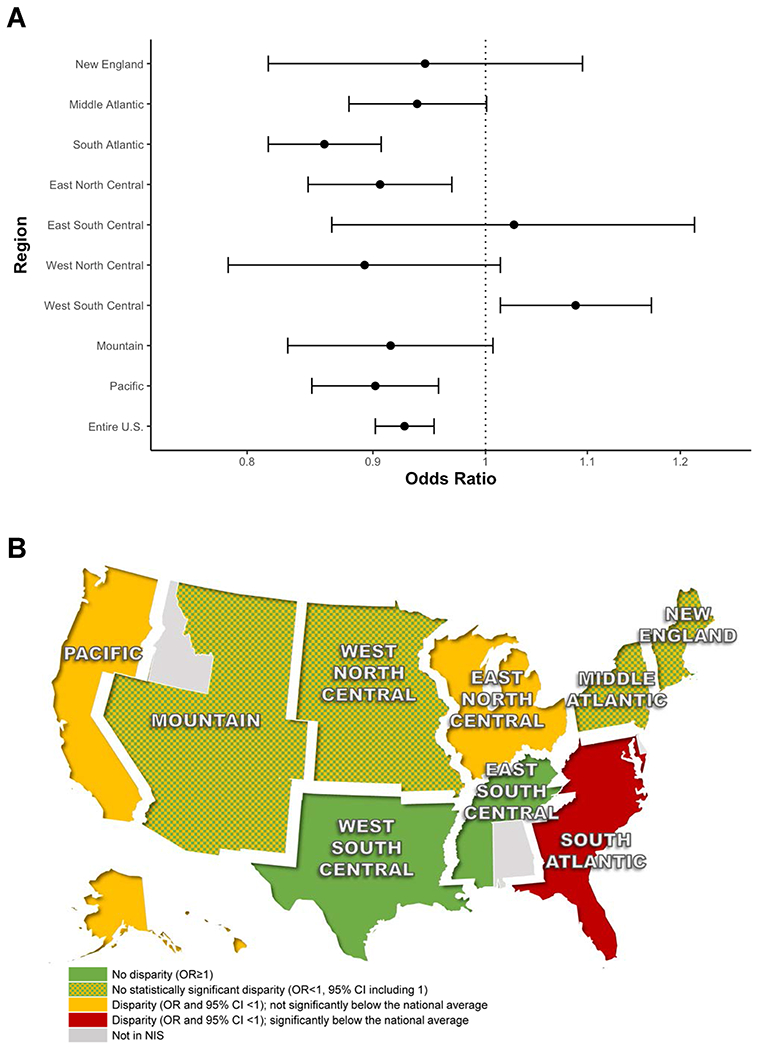
Results: Of the 545 509 included cases, 47 031 (8.6%) received IVT. Racially/ethnically minoritized groups had significantly lower adjusted odds of IVT compared with White people in the South Atlantic region (odds ratio [OR], 0.86 [95% CI, 0.82-0.91]), the East North Central region (OR, 0.91 [95% CI, 0.85-0.97]) and the Pacific region (OR, 0.90 [95% CI, 0.85-0.96]). In the South Atlantic region, IVT use in racial/ethnic minority groups was below the national average of all racial/ethnic minority patients (P=0.002). Compared with White patients, Black patients had lower odds of IVT in the Middle Atlantic region (OR, 0.84 [95% CI, 0.78-0.91]), the South Atlantic region (OR, 0.78 [95% CI, 0.74-0.82]), and the East North Central region (OR, 0.86 [95% CI, 0.79-0.93]). In the South Atlantic region, this difference was below the national average for Black people (P<0.001). Hispanic patients had significantly lower use of IVT only in the Pacific region (OR, 0.92 [95% CI, 0.85-0.99]), while Asian/Pacific Islander patients had lower odds of IVT in the Mountain (OR, 0.76 [95% CI, 0.59-0.98]) and Pacific region (OR, 0.89 [95% CI, 0.82-0.97]).
Conclusions: Racial/ethnic disparities in IVT use in the United States vary by region. Geographic hotspots of lower IVT use in racially/ethnically minoritized groups are the South Atlantic region, driven predominantly by lower use of IVT in Black patients, and the East North Central and Pacific regions.
Keywords: African Americans; ethnic groups; geographic locations; minority groups; stroke; thrombolytic therapy.
Figures

References
-
- Sacco RL, Gardener H, Wang K, Dong C, Ciliberti-Vargas MA, Gutierrez CM, Asdaghi N, Burgin WS, Carrasquillo O, Garcia-Rivera EJ, et al. Racial-Ethnic Disparities in Acute Stroke Care in the Florida-Puerto Rico Collaboration to Reduce Stroke Disparities Study. J Am Heart Assoc. 2017;6. doi: 10.1161/JAHA.116.004073 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
