

COVID-19 pneumonia: pathophysiology and management
- PMID: 34670808
- PMCID: PMC8527244
- DOI: 10.1183/16000617.0138-2021
COVID-19 pneumonia: pathophysiology and management
Abstract
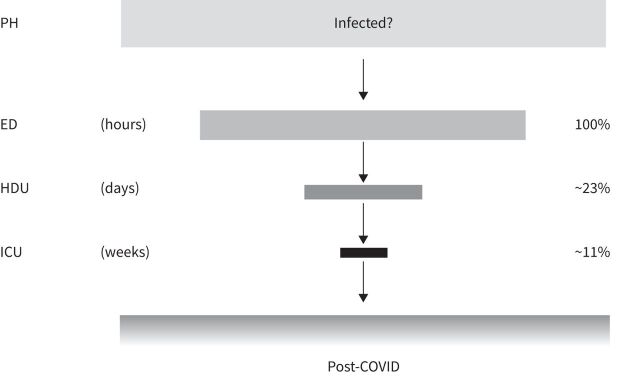
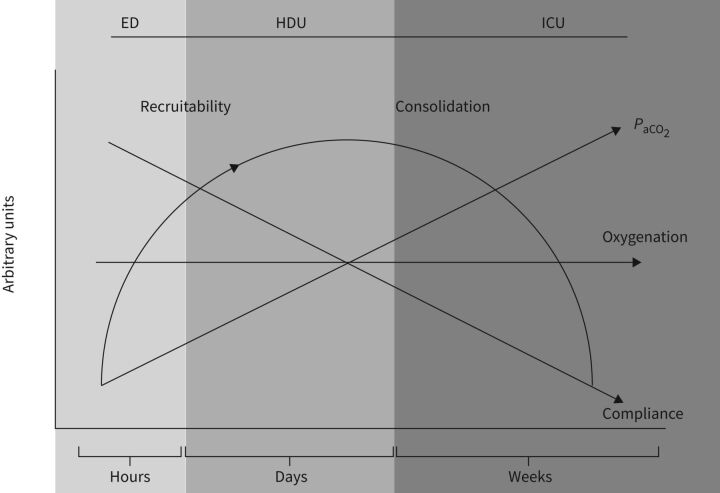
Coronavirus disease 2019 (COVID-19) pneumonia is an evolving disease. We will focus on the development of its pathophysiologic characteristics over time, and how these time-related changes determine modifications in treatment. In the emergency department: the peculiar characteristic is the coexistence, in a significant fraction of patients, of severe hypoxaemia, near-normal lung computed tomography imaging, lung gas volume and respiratory mechanics. Despite high respiratory drive, dyspnoea and respiratory rate are often normal. The underlying mechanism is primarily altered lung perfusion. The anatomical prerequisites for PEEP (positive end-expiratory pressure) to work (lung oedema, atelectasis, and therefore recruitability) are lacking. In the high-dependency unit: the disease starts to worsen either because of its natural evolution or additional patient self-inflicted lung injury (P-SILI). Oedema and atelectasis may develop, increasing recruitability. Noninvasive supports are indicated if they result in a reversal of hypoxaemia and a decreased inspiratory effort. Otherwise, mechanical ventilation should be considered to avert P-SILI. In the intensive care unit: the primary characteristic of the advance of unresolved COVID-19 disease is a progressive shift from oedema or atelectasis to less reversible structural lung alterations to lung fibrosis. These later characteristics are associated with notable impairment of respiratory mechanics, increased arterial carbon dioxide tension (P aCO2 ), decreased recruitability and lack of response to PEEP and prone positioning.
Copyright ©The authors 2021.
Conflict of interest statement
Conflicts of interest: L. Gattinoni reports consultancy fee from General Electrics and SIDAM. He also received lecture fees from Estor and Dimar. Conflicts of interest: S. Gattarello has nothing to disclose. Conflicts of interest: I. Steinberg has nothing to disclose. Conflicts of interest: M. Busana has nothing to disclose. Conflicts of interest: P. Palermo has nothing to disclose. Conflicts of interest: S. Lazzari has nothing to disclose. Conflicts of interest: F. Romitti has nothing to disclose. Conflicts of interest: M. Quintel has nothing to disclose. Conflicts of interest: K. Meissner has nothing to disclose. Conflicts of interest: J.J. Marini has nothing to disclose. Conflicts of interest: D. Chiumello has nothing to disclose. Conflicts of interest: L. Camporota has nothing to disclose.
Figures

Comment in
-
Hypoxaemia in COVID-19: many pieces to a complex puzzle.Eur Respir Rev. 2022 Jun 28;31(164):220090. doi: 10.1183/16000617.0090-2022. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35768129 Free PMC article.
-
Ventilation/perfusion mismatch is not the sole reason for hypoxaemia in early stage COVID-19 patients.Eur Respir Rev. 2022 Jun 28;31(164):210277. doi: 10.1183/16000617.0277-2021. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35768132 Free PMC article.
References
-
- WHO . WHO Coronavirus (COVID-19) Dashboard. http://covid19.who.int Date last accessed: June 17, 2021.
-
- Remap-Cap . REMAP-CAP . www.remapcap.org Date last accessed: June 15, 2021.
-
- Johns Hopkins University of Medicine . Coronavirus Resource Centre. https://coronavirus.jhu.edu Date last accessed: June 15, 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical