

Spared perilesional V1 activity underlies training-induced recovery of luminance detection sensitivity in cortically-blind patients
- PMID: 34671032
- PMCID: PMC8528839
- DOI: 10.1038/s41467-021-26345-1
Spared perilesional V1 activity underlies training-induced recovery of luminance detection sensitivity in cortically-blind patients
Abstract
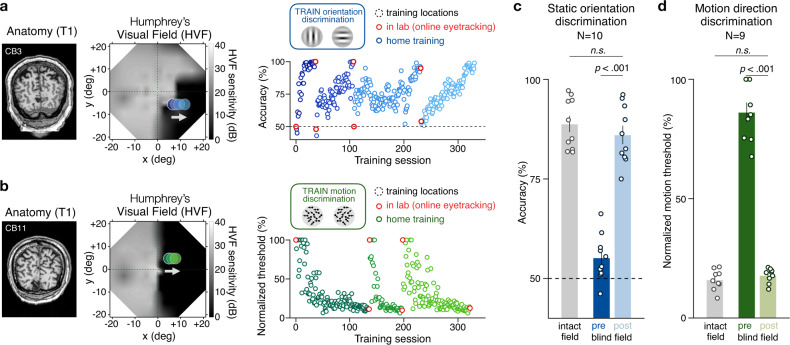
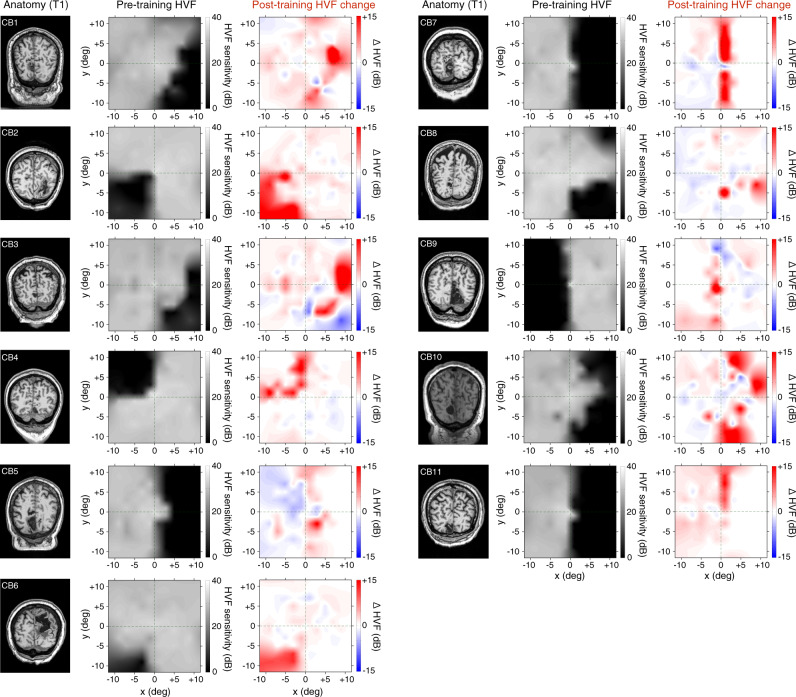
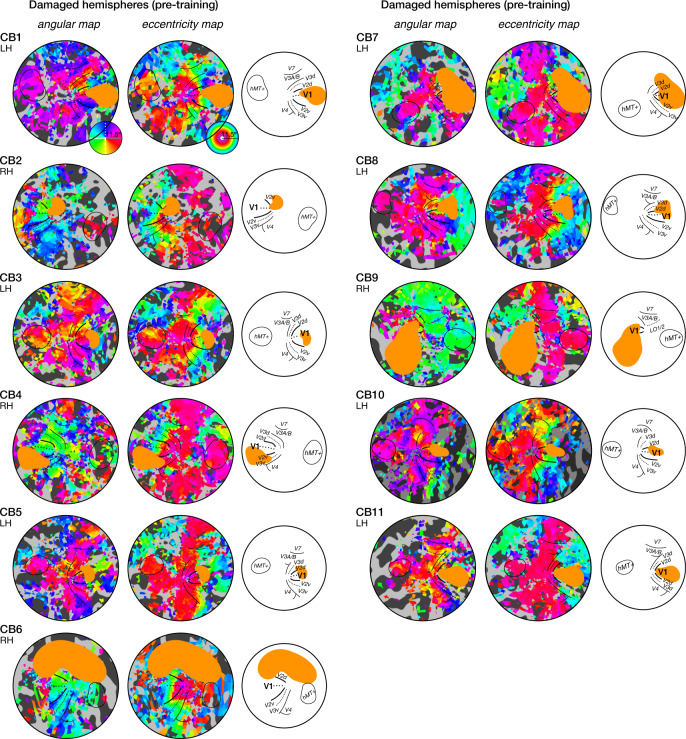
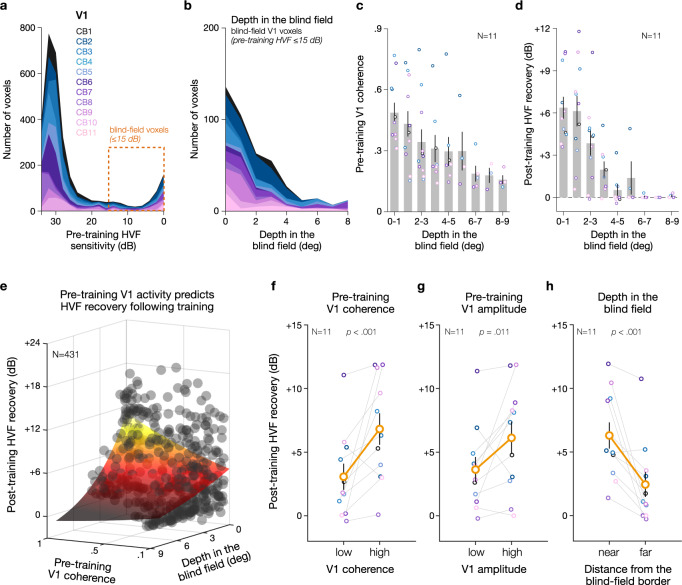
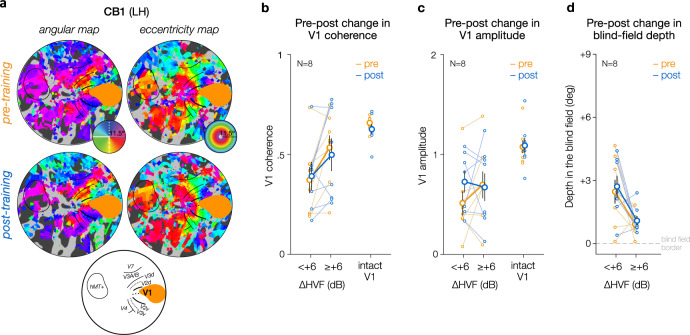
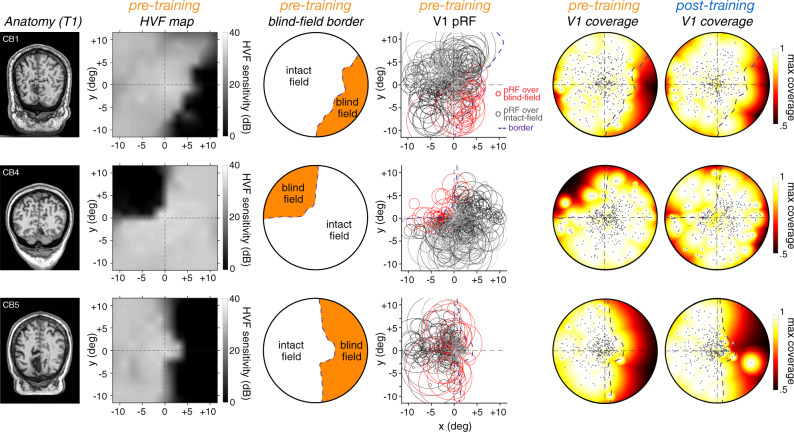
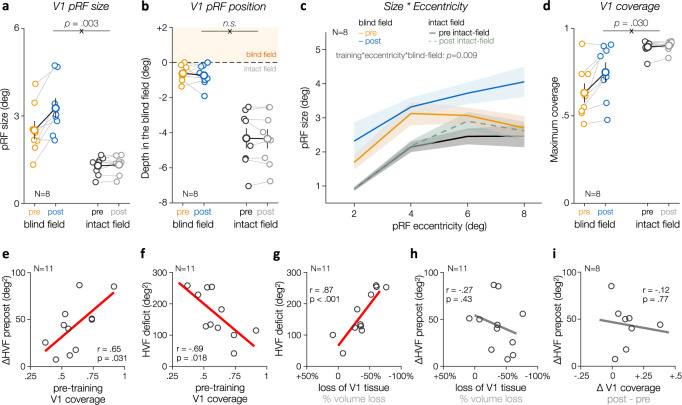
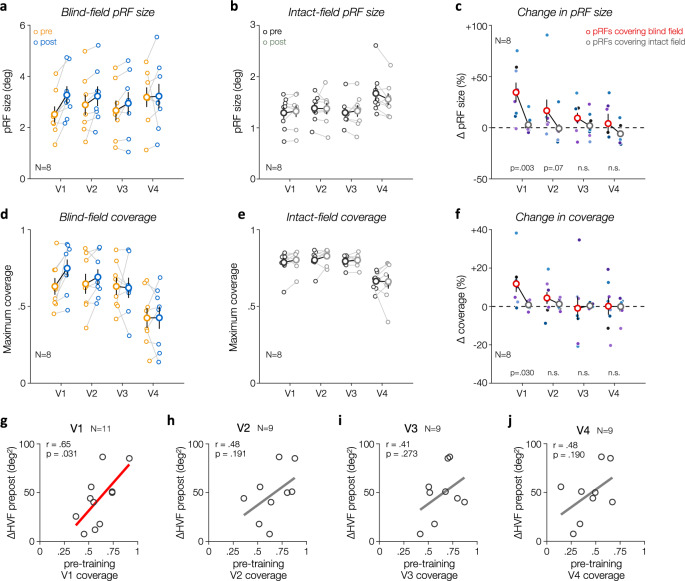
Damage to the primary visual cortex (V1) causes homonymous visual-field loss long considered intractable. Multiple studies now show that perceptual training can restore visual functions in chronic cortically-induced blindness (CB). A popular hypothesis is that training can harness residual visual functions by recruiting intact extrageniculostriate pathways. Training may also induce plastic changes within spared regions of the damaged V1. Here, we link changes in luminance detection sensitivity with retinotopic fMRI activity before and after visual discrimination training in eleven patients with chronic, stroke-induced CB. We show that spared V1 activity representing perimetrically-blind locations prior to training predicts the amount of training-induced recovery of luminance detection sensitivity. Additionally, training results in an enlargement of population receptive fields in perilesional V1, which increases blind-field coverage and may support further recovery with subsequent training. These findings uncover fundamental changes in perilesional V1 cortex underlying training-induced restoration of conscious luminance detection sensitivity in CB.
© 2021. The Author(s).
Conflict of interest statement
KRH is co-inventor on US Patent No. 7,549,743. The remaining authors have no competing interests.
Figures
References
-
- Pollock, A. et al. Interventions for visual field defects in patients with stroke. Cochrane Database Syst. Rev. CD008388 10.1002/14651858.CD008388.pub2 (2011). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
