

Some Patients Are More Equal Than Others: Variation in Ventilator Settings for Coronavirus Disease 2019 Acute Respiratory Distress Syndrome
- PMID: 34671747
- PMCID: PMC8522869
- DOI: 10.1097/CCE.0000000000000555
Some Patients Are More Equal Than Others: Variation in Ventilator Settings for Coronavirus Disease 2019 Acute Respiratory Distress Syndrome
Abstract
Objectives: As coronavirus disease 2019 is a novel disease, treatment strategies continue to be debated. This provides the intensive care community with a unique opportunity as the population of coronavirus disease 2019 patients requiring invasive mechanical ventilation is relatively homogeneous compared with other ICU populations. We hypothesize that the novelty of coronavirus disease 2019 and the uncertainty over its similarity with noncoronavirus disease 2019 acute respiratory distress syndrome resulted in substantial practice variation between hospitals during the first and second waves of coronavirus disease 2019 patients.
Design: Multicenter retrospective cohort study.
Setting: Twenty-five hospitals in the Netherlands from February 2020 to July 2020, and 14 hospitals from August 2020 to December 2020.
Patients: One thousand two hundred ninety-four critically ill intubated adult ICU patients with coronavirus disease 2019 were selected from the Dutch Data Warehouse. Patients intubated for less than 24 hours, transferred patients, and patients still admitted at the time of data extraction were excluded.
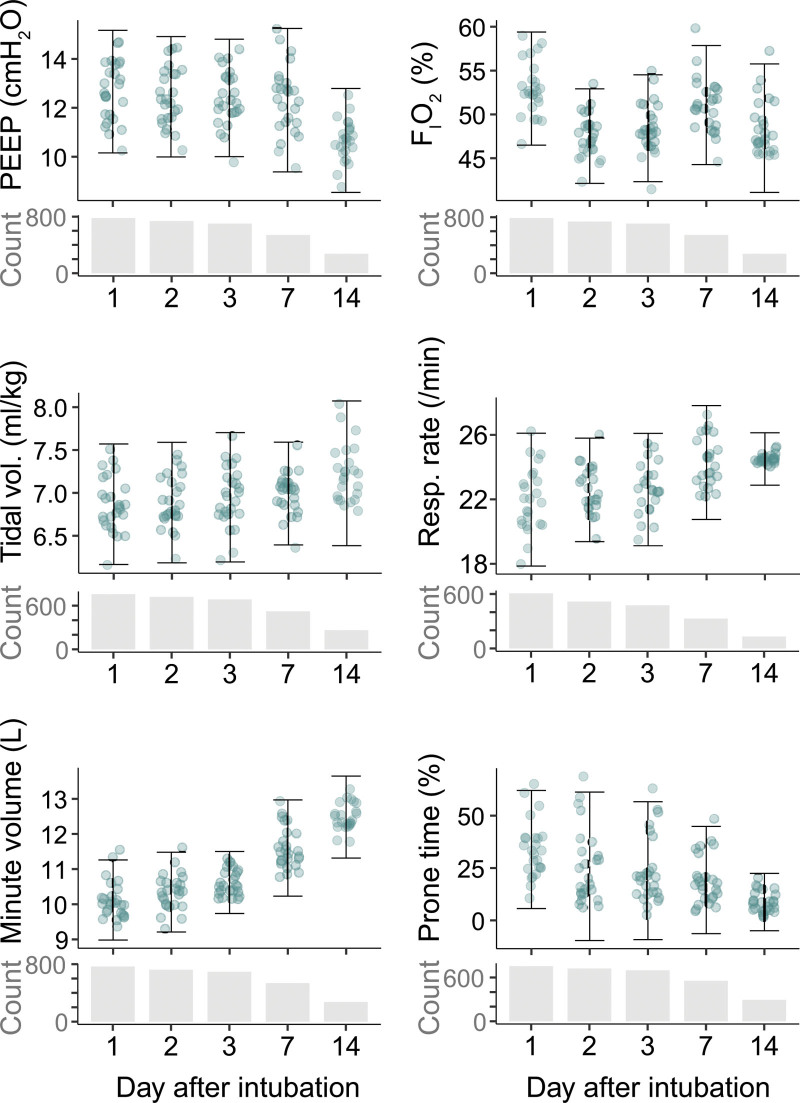
Measurements and main results: We aimed to estimate between-ICU practice variation in selected ventilation parameters (positive end-expiratory pressure, Fio2, set respiratory rate, tidal volume, minute volume, and percentage of time spent in a prone position) on days 1, 2, 3, and 7 of intubation, adjusted for patient characteristics as well as severity of illness based on Pao2/Fio2 ratio, pH, ventilatory ratio, and dynamic respiratory system compliance during controlled ventilation. Using multilevel linear mixed-effects modeling, we found significant (p ≤ 0.001) variation between ICUs in all ventilation parameters on days 1, 2, 3, and 7 of intubation for both waves.
Conclusions: This is the first study to clearly demonstrate significant practice variation between ICUs related to mechanical ventilation parameters that are under direct control by intensivists. Their effect on clinical outcomes for both coronavirus disease 2019 and other critically ill mechanically ventilated patients could have widespread implications for the practice of intensive care medicine and should be investigated further by causal inference models and clinical trials.
Keywords: acute respiratory distress syndrome; clinical practice variation; coronavirus disease 2019; mechanical ventilation.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures


References
-
- Alhazzani W, Evans L, Alshamsi F, et al. . Surviving sepsis campaign guidelines on the management of adults with coronavirus disease 2019 (COVID-19) in the ICU: First update. Crit Care Med. 2021; 49:e219–e234 - PubMed
-
- von Elm E, Altman DG, Egger M, et al. ; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet. 2007; 370:1453–1457 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
