

This is a preprint.
Heterologous SARS-CoV-2 Booster Vaccinations - Preliminary Report
- PMID: 34671773
- PMCID: PMC8528081
- DOI: 10.1101/2021.10.10.21264827
Heterologous SARS-CoV-2 Booster Vaccinations - Preliminary Report
Update in
- This article has been published with doi: 10.1056/nejmoa2116414 doi: 10.1056/nejmoa2116414
Abstract
Background: While Coronavirus disease 2019 (Covid-19) vaccines are highly effective, breakthrough infections are occurring. Booster vaccinations have recently received emergency use authorization (EUA) for certain populations but are restricted to homologous mRNA vaccines. We evaluated homologous and heterologous booster vaccination in persons who had received an EUA Covid-19 vaccine regimen.
Methods: In this phase 1/2 open-label clinical trial conducted at ten U.S. sites, adults who received one of three EUA Covid-19 vaccines at least 12 weeks prior to enrollment and had no reported history of SARS-CoV-2 infection received a booster injection with one of three vaccines (Moderna mRNA-1273 100-μg, Janssen Ad26.COV2.S 5×1010 virus particles, or Pfizer-BioNTech BNT162b2 30-μg; nine combinations). The primary outcomes were safety, reactogenicity, and humoral immunogenicity on study days 15 and 29.
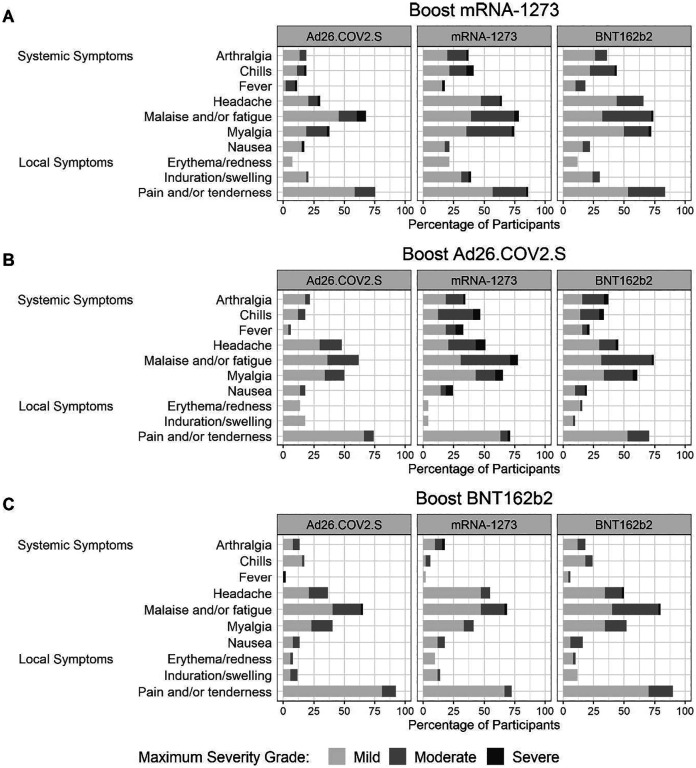
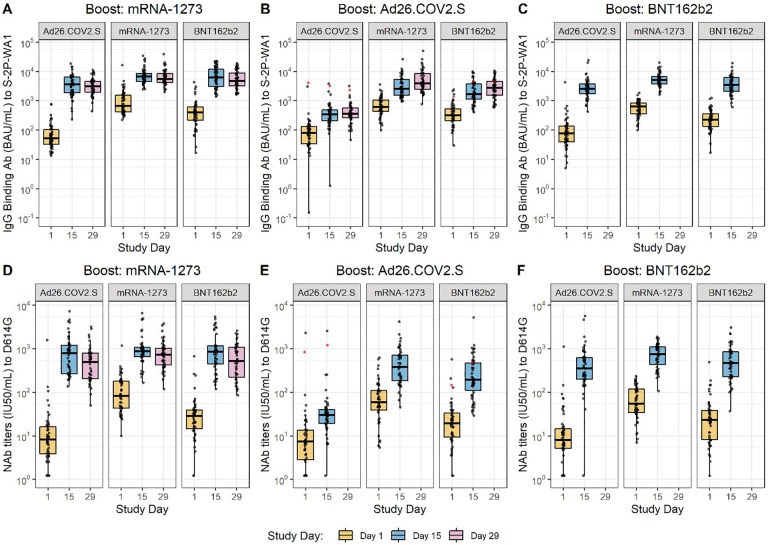
Results: 458 individuals were enrolled: 154 received mRNA-1273, 150 received Ad26.CoV2.S, and 153 received BNT162b2 booster vaccines. Reactogenicity was similar to that reported for the primary series. Injection site pain, malaise, headache, and myalgia occurred in more than half the participants. Booster vaccines increased the neutralizing activity against a D614G pseudovirus (4.2-76-fold) and binding antibody titers (4.6-56-fold) for all combinations; homologous boost increased neutralizing antibody titers 4.2-20-fold whereas heterologous boost increased titers 6.2-76-fold. Day 15 neutralizing and binding antibody titers varied by 28.7-fold and 20.9-fold, respectively, across the nine prime-boost combinations.
Conclusion: Homologous and heterologous booster vaccinations were well-tolerated and immunogenic in adults who completed a primary Covid-19 vaccine regimen at least 12 weeks earlier.
Keywords: Booster; Covid-19; SARS-CoV-2; Vaccine; antibody; mRNA; recombinant adenovirus.
Figures
References
-
- CDC. COVID Data Tracker: COVID-19 Vaccinations in the United States. https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-total-admin-.... Accessed October 9, 2021.
-
- Brown CM, Vostok J, Johnson H, Burns M, Gharpure R, Sami S, et al. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings - Barnstable County, Massachusetts, July 2021. MMWR Morb Mortal Wkly Rep 2021;70(31):1059–1062. DOI: 10.15585/mmwr.mm7031e2. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous