Factors influencing the levothyroxine dose in the hormone replacement therapy of primary hypothyroidism in adults
- PMID: 34671932
- PMCID: PMC8528480
- DOI: 10.1007/s11154-021-09691-9
Factors influencing the levothyroxine dose in the hormone replacement therapy of primary hypothyroidism in adults
Abstract
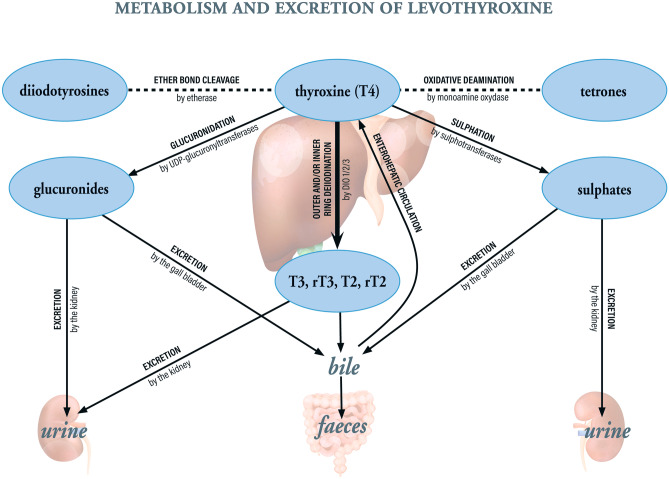
Levothyroxine (LT4) is a safe, effective means of hormone replacement therapy for hypothyroidism. Here, we review the pharmaceutical, pathophysiological and behavioural factors influencing the absorption, distribution, metabolism and excretion of LT4. Any factor that alters the state of the epithelium in the stomach or small intestine will reduce and/or slow absorption of LT4; these include ulcerative colitis, coeliac disease, bariatric surgery, Helicobacter pylori infection, food intolerance, gastritis, mineral supplements, dietary fibre, resins, and various drugs. Once in the circulation, LT4 is almost fully bound to plasma proteins. Although free T4 (FT4) and liothyronine concentrations are extensively buffered, it is possible that drug- or disorder-induced changes in plasma proteins levels can modify free hormone levels. The data on the clinical significance of genetic variants in deiodinase genes are contradictory, and wide-scale genotyping of hypothyroid patients is not currently justified. We developed a decision tree for the physician faced with an abnormally high thyroid-stimulating hormone (TSH) level in a patient reporting adequate compliance with the recommended LT4 dose. The physician should review medications, the medical history and the serum FT4 level and check for acute adrenal insufficiency, heterophilic anti-TSH antibodies, antibodies against gastric and intestinal components (gastric parietal cells, endomysium, and tissue transglutaminase 2), and Helicobacter pylori infection. The next step is an LT4 pharmacodynamic absorption test; poor LT4 absorption should prompt a consultation with a gastroenterologist and (depending on the findings) an increase in the LT4 dose level. An in-depth etiological investigation can reveal visceral disorders and, especially, digestive tract disorders.
Keywords: Absorption; Deiodinases; Drugs; LT4 absorption test; Metabolism; Pseudomalabsorption.
© 2021. The Author(s).
Conflict of interest statement
Philippe Caron has received consulting fees, honoraria for lectures and/or research funding from Merck Serono SAS and Laboratoires Genevrier; Solange Grunenwald has received consulting fees, honoraria for lectures and/or research funding from Merck Serono SAS, ESAI France, and Ipsen France; Luca Persani has received consulting fees, honoraria for lectures and/or research funding from Merck Serono and Sandoz Italy; Françoise Borson-Chazot has received consulting fees, honoraria for lectures and/or research funding from Merck Serono SAS and ESAI France; Remy Leroy has received consulting fees, honoraria for lectures and/or research funding from Merck Serono SAS; Leonidas Duntas has received consulting fees, honoraria for lectures and/or research funding from Merck Serono and Berlin-Chemie.
Figures