

The potential and limitations of intrahepatic cholangiocyte organoids to study inborn errors of metabolism
- PMID: 34671987
- PMCID: PMC9298016
- DOI: 10.1002/jimd.12450
The potential and limitations of intrahepatic cholangiocyte organoids to study inborn errors of metabolism
Abstract
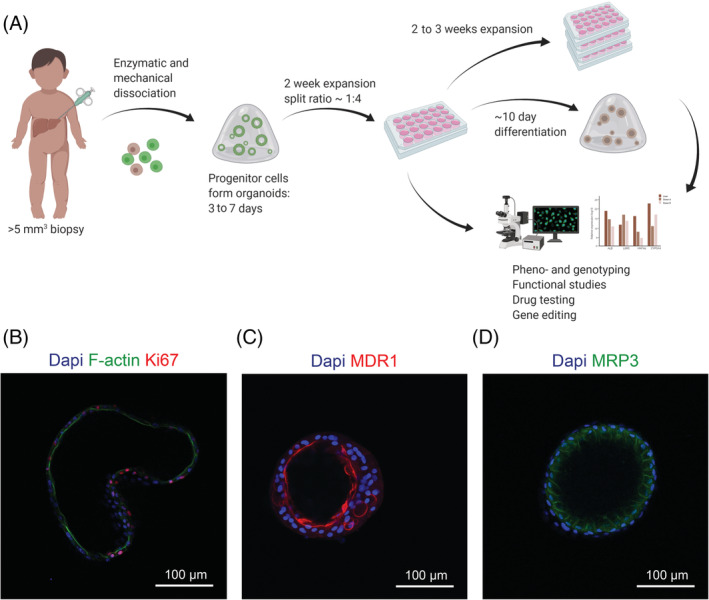
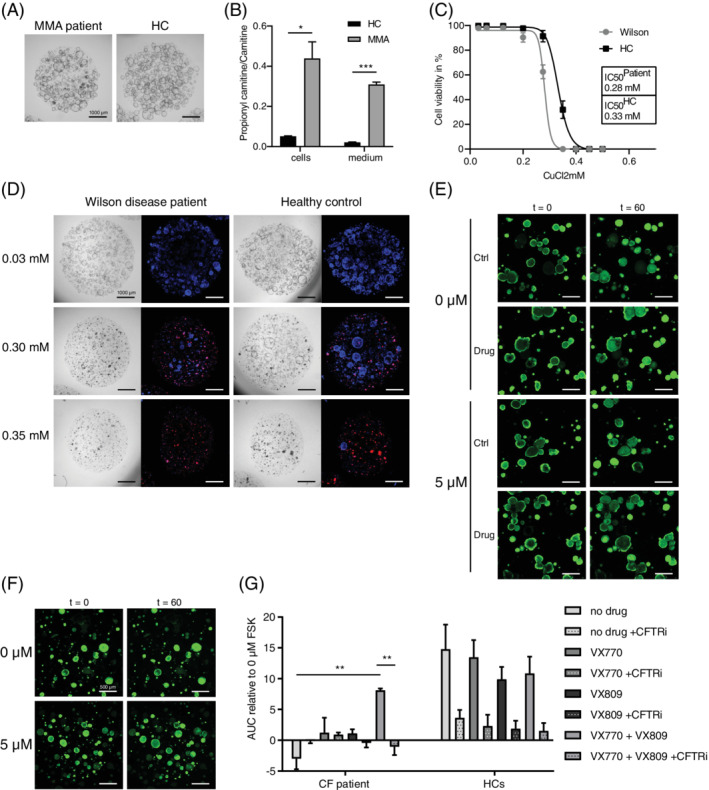
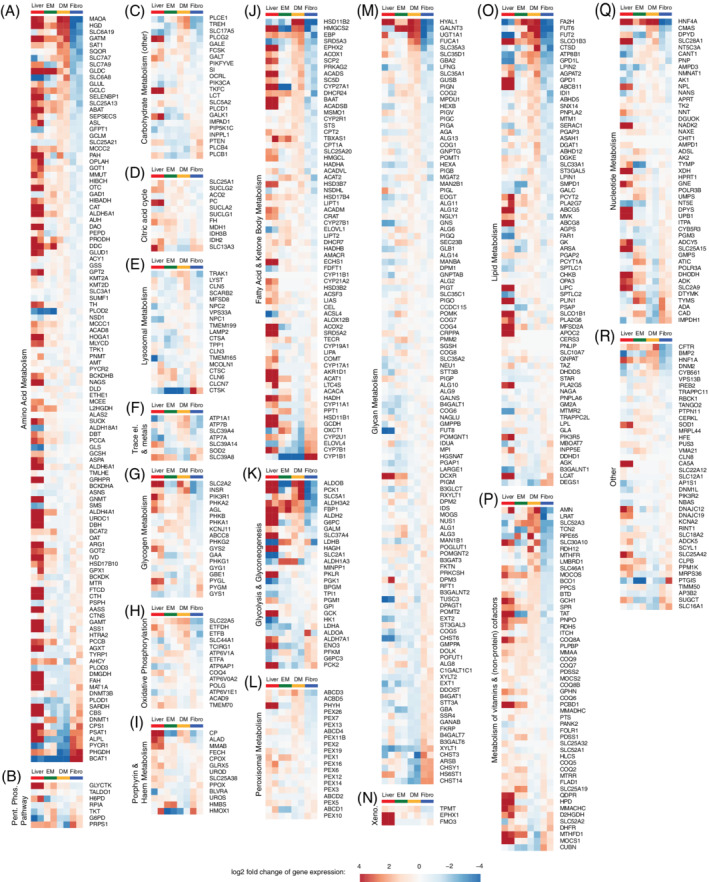
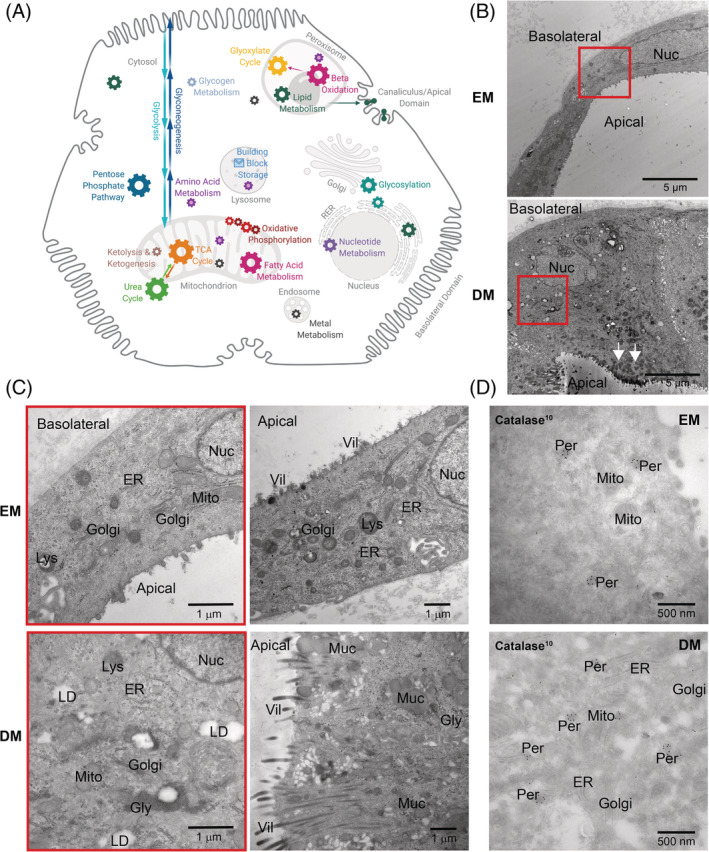
Inborn errors of metabolism (IEMs) comprise a diverse group of individually rare monogenic disorders that affect metabolic pathways. Mutations lead to enzymatic deficiency or dysfunction, which results in intermediate metabolite accumulation or deficit leading to disease phenotypes. Currently, treatment options for many IEMs are insufficient. Rarity of individual IEMs hampers therapy development and phenotypic and genetic heterogeneity suggest beneficial effects of personalized approaches. Recently, cultures of patient-own liver-derived intrahepatic cholangiocyte organoids (ICOs) have been established. Since most metabolic genes are expressed in the liver, patient-derived ICOs represent exciting possibilities for in vitro modeling and personalized drug testing for IEMs. However, the exact application range of ICOs remains unclear. To address this, we examined which metabolic pathways can be studied with ICOs and what the potential and limitations of patient-derived ICOs are to model metabolic functions. We present functional assays in patient ICOs with defects in branched-chain amino acid metabolism (methylmalonic acidemia), copper metabolism (Wilson disease), and transporter defects (cystic fibrosis). We discuss the broad range of functional assays that can be applied to ICOs, but also address the limitations of these patient-specific cell models. In doing so, we aim to guide the selection of the appropriate cell model for studies of a specific disease or metabolic process.
Keywords: Wilson disease; cystic fibrosis; inborn errors of metabolism; intrahepatic cholangiocyte organoids; methylmalonic acidemia; patient-specific in vitro modeling.
© 2021 The Authors. Journal of Inherited Metabolic Disease published by John Wiley & Sons Ltd on behalf of SSIEM.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
